

Evidence for genetic heterogeneity between clinical subtypes of bipolar disorder
- PMID: 28072414
- PMCID: PMC5545718
- DOI: 10.1038/tp.2016.242
Evidence for genetic heterogeneity between clinical subtypes of bipolar disorder
Abstract
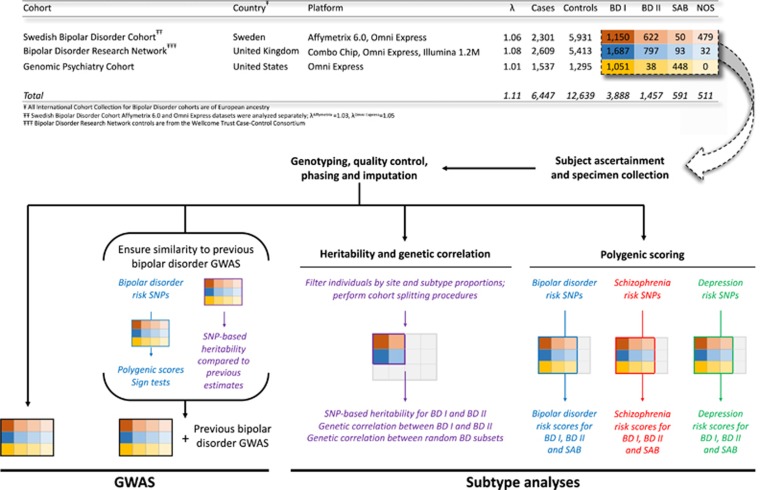
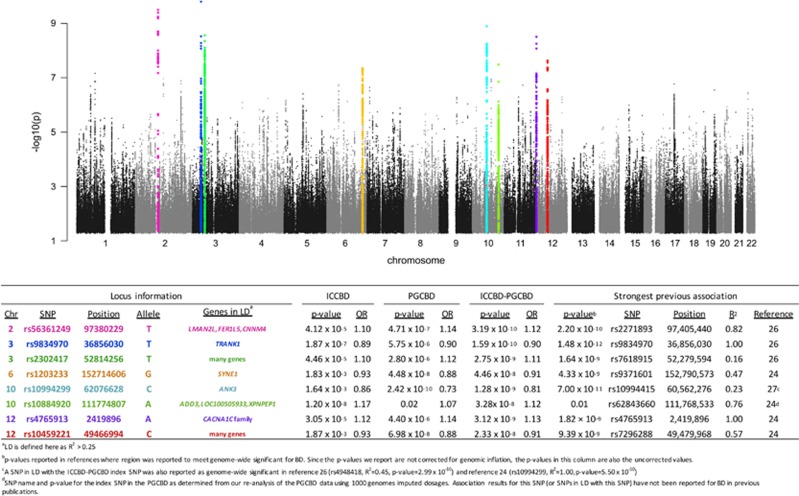
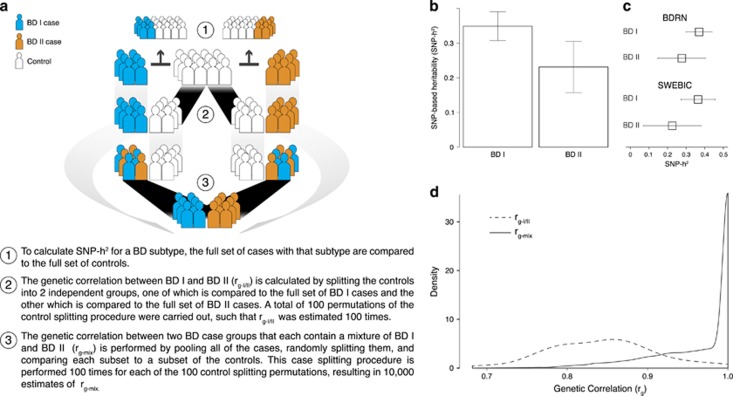
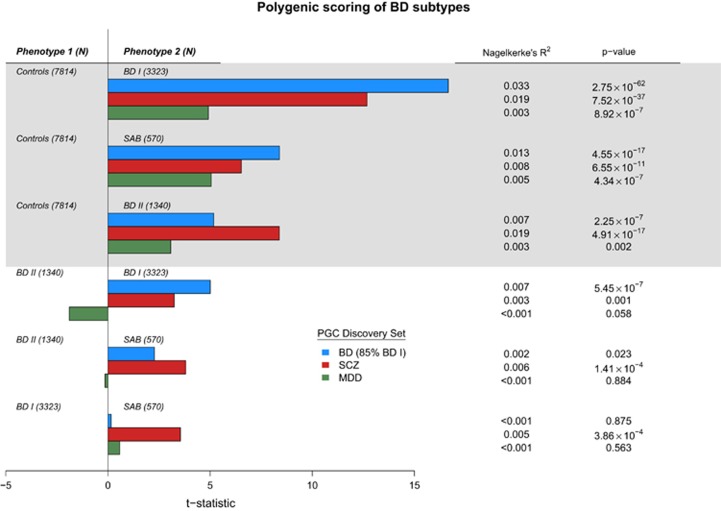
We performed a genome-wide association study of 6447 bipolar disorder (BD) cases and 12 639 controls from the International Cohort Collection for Bipolar Disorder (ICCBD). Meta-analysis was performed with prior results from the Psychiatric Genomics Consortium Bipolar Disorder Working Group for a combined sample of 13 902 cases and 19 279 controls. We identified eight genome-wide significant, associated regions, including a novel associated region on chromosome 10 (rs10884920; P=3.28 × 10-8) that includes the brain-enriched cytoskeleton protein adducin 3 (ADD3), a non-coding RNA, and a neuropeptide-specific aminopeptidase P (XPNPEP1). Our large sample size allowed us to test the heritability and genetic correlation of BD subtypes and investigate their genetic overlap with schizophrenia and major depressive disorder. We found a significant difference in heritability of the two most common forms of BD (BD I SNP-h2=0.35; BD II SNP-h2=0.25; P=0.02). The genetic correlation between BD I and BD II was 0.78, whereas the genetic correlation was 0.97 when BD cohorts containing both types were compared. In addition, we demonstrated a significantly greater load of polygenic risk alleles for schizophrenia and BD in patients with BD I compared with patients with BD II, and a greater load of schizophrenia risk alleles in patients with the bipolar type of schizoaffective disorder compared with patients with either BD I or BD II. These results point to a partial difference in the genetic architecture of BD subtypes as currently defined.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kraepelin E. Manic-Depressive Insanity and Paranoia. E. & S. Livingstone,1921.
-
- Leonhard K. Pathogenesis of manic-depressive disease. Der Nervenarzt 1957; 28: 271–272. - PubMed
-
- Dunner DL, Gershon ES, Goodwin FK. Heritable factors in the severity of affective illness. Biol Psychiatry 1976; 11: 31–42. - PubMed
-
- Fieve RR, Kumbaraci T, Dunner DL. Lithium prophylaxis of depression in bipolar I, bipolar II, and unipolar patients. Am J Psychiatry 1976; 133: 925–929. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
