

The impact of overdiagnosis on the selection of efficient lung cancer screening strategies
- PMID: 28073150
- PMCID: PMC5516788
- DOI: 10.1002/ijc.30602
The impact of overdiagnosis on the selection of efficient lung cancer screening strategies
Abstract
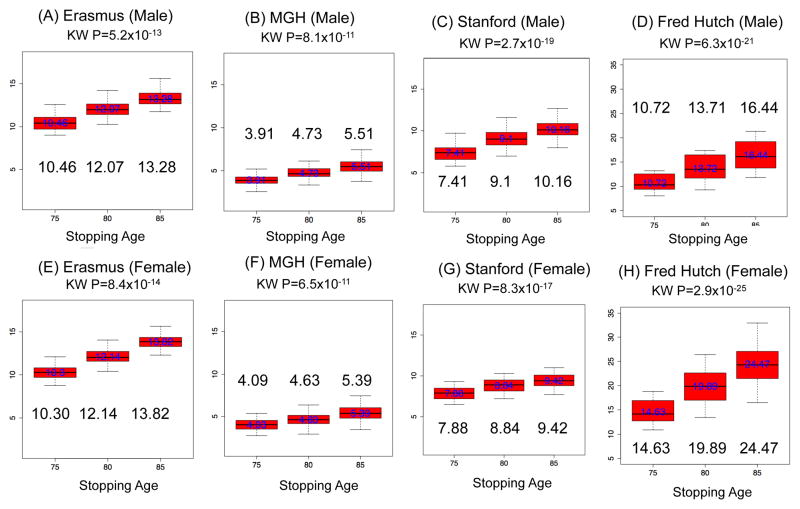
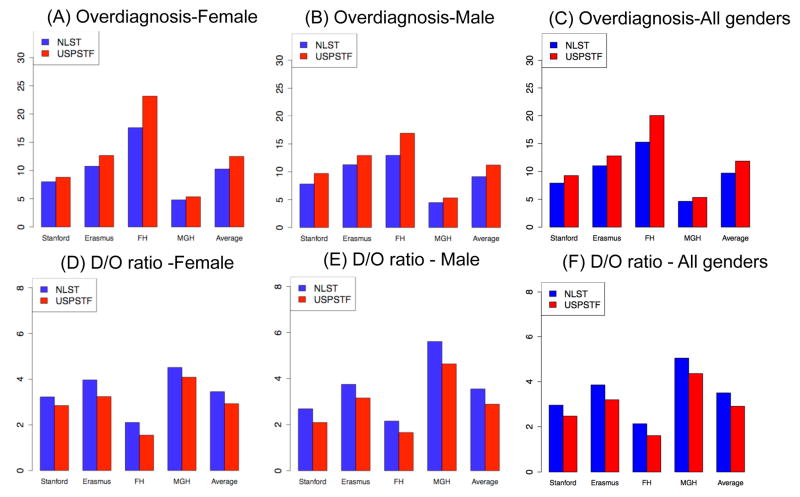
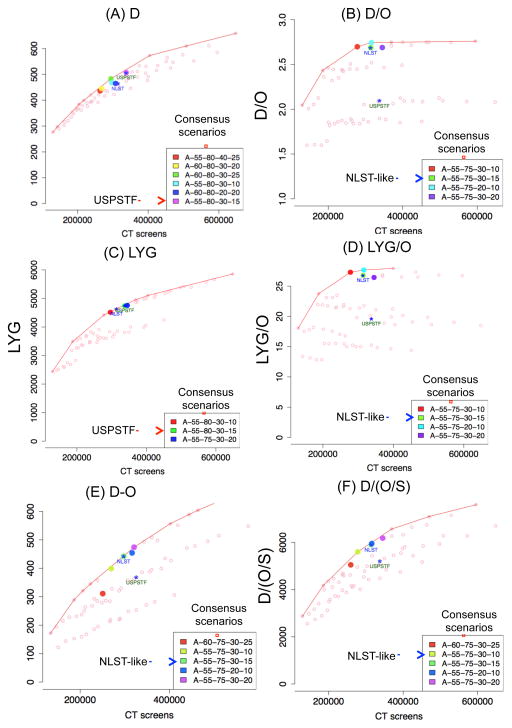
The U.S. Preventive Services Task Force (USPSTF) recently updated their national lung screening guidelines and recommended low-dose computed tomography (LDCT) for lung cancer (LC) screening through age 80. However, the risk of overdiagnosis among older populations is a concern. Using four comparative models from the Cancer Intervention and Surveillance Modeling Network, we evaluate the overdiagnosis of the screening program recommended by USPSTF in the U.S. 1950 birth cohort. We estimate the number of LC deaths averted by screening (D) per overdiagnosed case (O), yielding the ratio D/O, to quantify the trade-off between the harms and benefits of LDCT. We analyze 576 hypothetical screening strategies that vary by age, smoking, and screening frequency and evaluate efficient screening strategies that maximize the D/O ratio and other metrics including D and life-years gained (LYG) per overdiagnosed case. The estimated D/O ratio for the USPSTF screening program is 2.85 (model range: 1.5-4.5) in the 1950 birth cohort, implying LDCT can prevent ∼3 LC deaths per overdiagnosed case. This D/O ratio increases by 22% when the program stops screening at an earlier age 75 instead of 80. Efficiency frontier analysis shows that while the most efficient screening strategies that maximize the mortality reduction (D) irrespective of overdiagnosis screen through age 80, screening strategies that stop at age 75 versus 80 produce greater efficiency in increasing life-years gained per overdiagnosed case. Given the risk of overdiagnosis with LC screening, the stopping age of screening merits further consideration when balancing benefits and harms.
Keywords: USPSTF; computed tomography; health policy; lung cancer; lung cancer screening; microsimulation; overdiagnosis; simulation model.
© 2017 UICC.
Conflict of interest statement
Competing Interests
HJdK took part in a 1-day advisory meeting on biomarkers organized by M.D.
Anderson/Health Sciences during the 16th World Conference on Lung Cancer.
HJdK and KtH received a grant from the University of Zurich to assess the cost-effectiveness of computed tomographic lung cancer screening in Switzerland
Figures
Comment in
-
Think before you leap.Int J Cancer. 2018 Apr 1;142(7):1505-1506. doi: 10.1002/ijc.31185. Epub 2017 Dec 28. Int J Cancer. 2018. PMID: 29194602 No abstract available.
References
-
- Dammas S, Patz EF, Jr, Goodman PC. Identification of small lung nodules at autopsy: implications for lung cancer screening and overdiagnosis bias. Lung Cancer. 2001;33:11–16. - PubMed
-
- Black WC. Overdiagnosis: an underrecognized cause of confusion and harm in cancer screening. Journal of the National Cancer Institute. 2000;92:1280–82. - PubMed
-
- Welch HG, Black WC. Overdiagnosis in cancer. Journal of the National Cancer Institute. 2010;102:605–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
