

Characterizing Pharmacogenomic-Guided Medication Use With a Clinical Data Repository
- PMID: 28073152
- PMCID: PMC5503815
- DOI: 10.1002/cpt.611
Characterizing Pharmacogenomic-Guided Medication Use With a Clinical Data Repository
Abstract
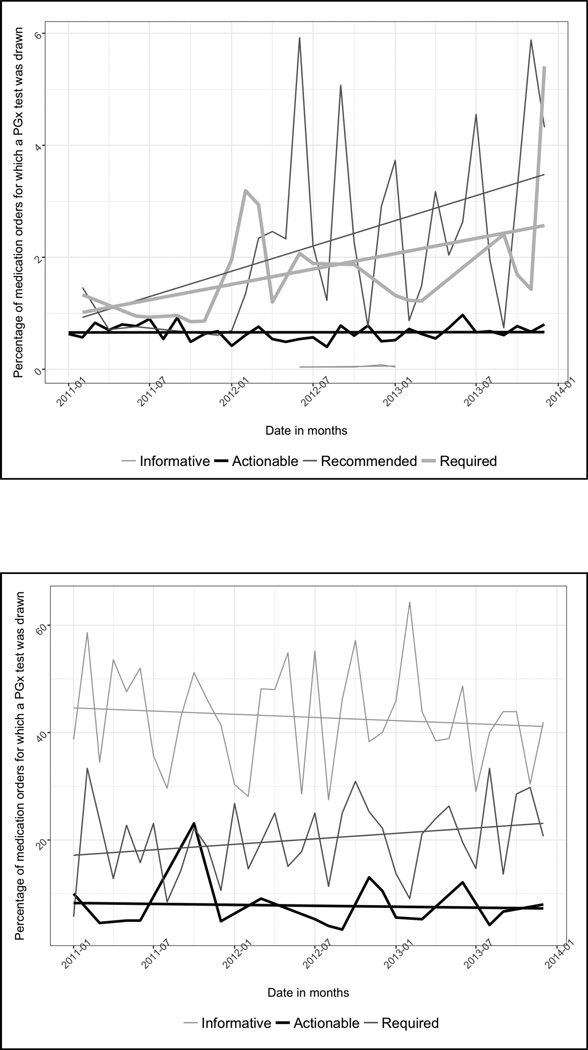
The extent to which pharmacogenomic-guided medication use has been adopted in various health systems is unclear. To assess the uptake of pharmacogenomic-guided medication use, we determined its frequency across our health system, which does not have a structured testing program. Using a multisite clinical data repository, we identified adult patients' first prescribed medications between January 2011 and December 2013 and investigated the frequency of germline and somatic pharmacogenomic testing, by the Pharmacogenomics Knowledgebase level of the US Food and Drug Administration label information. There were 268,262 medication orders for drugs with germline pharmacogenomic testing information in their drug labels. Pharmacogenomic testing was detected for 1.5% (129/8,718) of medication orders with recommended or required testing. Of the 3,817 medication orders associated with somatic pharmacogenomic testing information in their drug labels, 20% (372/1,819) of required tests were detected. The low rates of detectable pharmacogenomic testing suggest that structured testing programs are required to achieve the success of precision medicine.
© 2017 American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
Patrick C. Mathias – I have nothing to disclose.
Nathaniel Hendrix – I have nothing to disclose.
Wei-Jhih Wang – I have nothing to disclose.
Katelyn Keyloun– I have nothing to disclose.
Maher Khelifi– I have nothing to disclose.
Peter Tarczy-Hornoch– I have nothing to disclose.
Beth Devine – I have nothing to disclose.
Figures
References
-
- Center for Drug Evaluation and Research Table of Pharmacogenomic Biomarkers in Drug Labeling. 2014
-
- Frueh F, et al. Pharmacogenomic Biomarker Information in Drug Labels Approved by the United States Food and Drug Administration: Prevalence of Related Drug Use. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 2008;28:992–998. - PubMed
-
- Stanek, et al. Adoption of Pharmacogenomic Testing by US Physicians: Results of a Nationwide Survey. Clinical Pharmacology & Therapeutics. 2012;91:450–458. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
