

Costs of Care for Hospitalized Children Associated With Preferred Language and Insurance Type
- PMID: 28073815
- PMCID: PMC5535794
- DOI: 10.1542/hpeds.2016-0051
Costs of Care for Hospitalized Children Associated With Preferred Language and Insurance Type
Abstract
Objective: The study goal was to determine whether preferred language for care and insurance type are associated with cost among hospitalized children.
Methods: A retrospective cohort study was conducted of inpatients at a freestanding children's hospital from January 2011 to December 2012. Patient information and hospital costs were obtained from administrative data. Cost differences according to language and insurance were calculated using multivariate generalized linear model estimates, allowing for language/insurance interaction effects. Models were also stratified according to medical complexity and length of stay (LOS) ≥3 days.
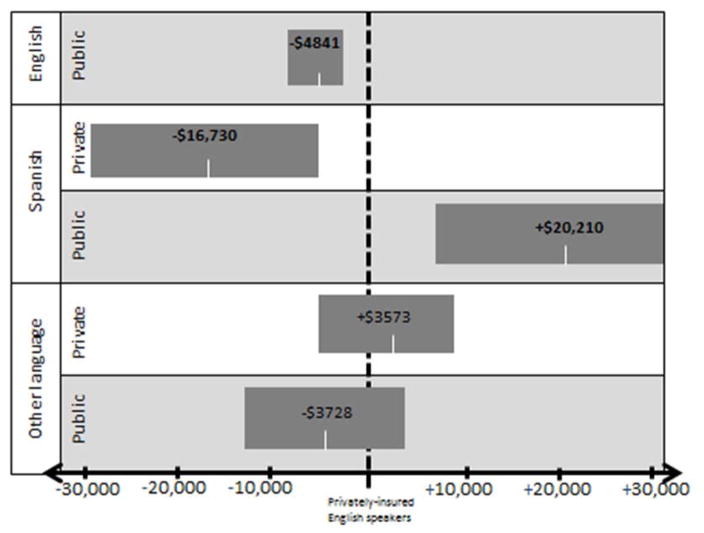
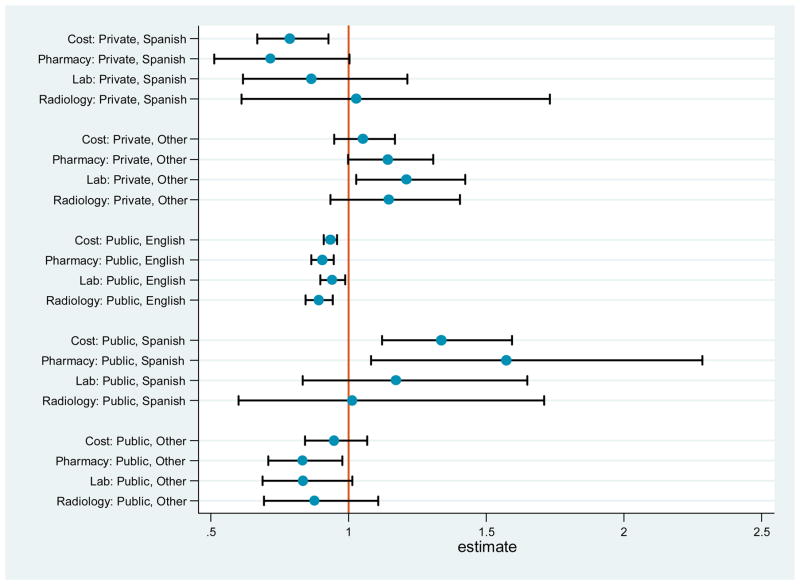
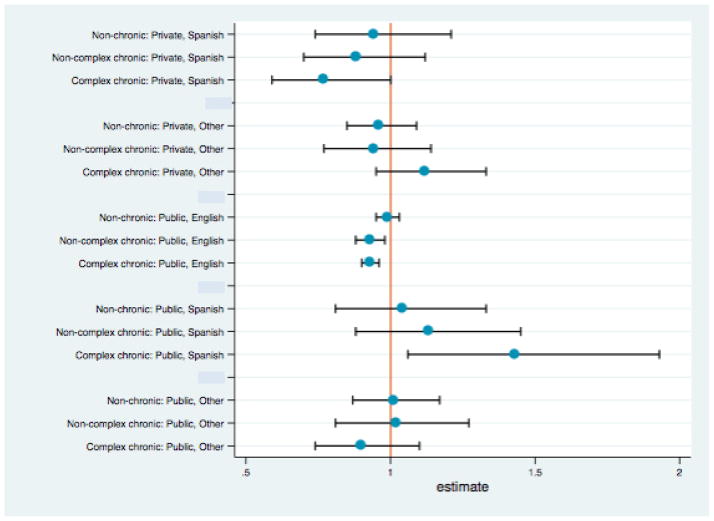
Results: Of 19 249 admissions, 8% of caregivers preferred Spanish and 6% preferred another language; 47% of admissions were covered by public insurance. Models controlled for LOS, medical complexity, home-to-hospital distance, age, asthma diagnosis, and race/ethnicity. Total hospital costs were significantly higher for publicly insured Spanish speakers ($20 211 [95% confidence interval (CI), 7781 to 32 641]) and lower for privately insured Spanish speakers (-$16 730 [95% CI, -28 265 to -5195]) and publicly insured English speakers (-$4841 [95% CI, -6781 to -2902]) compared with privately insured English speakers. Differences were most pronounced among children with medical complexity and LOS ≥3 days.
Conclusions: Hospital costs varied significantly according to preferred language and insurance type, even adjusting for LOS and medical complexity. These differences in the amount of billable care provided to medically similar patients may represent either underprovision or overprovision of care on the basis of sociodemographic factors and communication, suggesting problems with care efficiency and equity. Further investigation may inform development of effective interventions.
Copyright © 2017 by the American Academy of Pediatrics.
Conflict of interest statement
Figures
Similar articles
-
Comparison of length of stay for asthma by hospital type.Pediatrics. 1998 Apr;101(4):E13. doi: 10.1542/peds.101.4.e13. Pediatrics. 1998. PMID: 9521979
-
Lengths of stay and costs associated with children's hospitals.Pediatrics. 2005 Apr;115(4):839-44. doi: 10.1542/peds.2004-1622. Pediatrics. 2005. PMID: 15805353
-
Financial Loss for Inpatient Care of Medicaid-Insured Children.JAMA Pediatr. 2016 Nov 1;170(11):1055-1062. doi: 10.1001/jamapediatrics.2016.1639. JAMA Pediatr. 2016. PMID: 27618284
-
Language Barriers in Appendicitis: What is the Cost?Am Surg. 2025 May;91(5):871-876. doi: 10.1177/00031348251323710. Epub 2025 Feb 26. Am Surg. 2025. PMID: 40009870 Review.
-
Association of Demographics and Hospital Stay Characteristics With Patient Experience in Hospitalized Pediatric Patients.J Patient Exp. 2020 Dec;7(6):1077-1085. doi: 10.1177/2374373520925251. Epub 2020 May 19. J Patient Exp. 2020. PMID: 33457548 Free PMC article. Review.
Cited by
-
Sedation and analgesia doses do not differ across demographic factors in pediatric cardiac surgery patients.Front Pediatr. 2025 Jul 16;13:1577461. doi: 10.3389/fped.2025.1577461. eCollection 2025. Front Pediatr. 2025. PMID: 40740825 Free PMC article.
-
Completeness of Written Discharge Guidance for English- and Spanish-Speaking Patient Families.Hosp Pediatr. 2019 Jul;9(7):516-522. doi: 10.1542/hpeds.2018-0250. Epub 2019 Jun 10. Hosp Pediatr. 2019. PMID: 31182648 Free PMC article.
-
A sequential, multiple assignment randomized trial comparing web-based education to mobile video interpreter access for improving provider interpreter use in primary care clinics: the mVOCAL hybrid type 3 study protocol.Implement Sci. 2023 Mar 13;18(1):8. doi: 10.1186/s13012-023-01263-6. Implement Sci. 2023. PMID: 36915138 Free PMC article.
-
Identifying Modifiable Health Care Barriers to Improve Health Equity for Hospitalized Children.Hosp Pediatr. 2020 Jan;10(1):1-11. doi: 10.1542/hpeds.2019-0096. Epub 2019 Dec 4. Hosp Pediatr. 2020. PMID: 31801795 Free PMC article.
-
Inpatient Communication Barriers and Drivers When Caring for Limited English Proficiency Children.J Hosp Med. 2019 Oct 1;14(10):607-613. doi: 10.12788/jhm.3240. Epub 2019 Jul 24. J Hosp Med. 2019. PMID: 31339836 Free PMC article.
References
-
- Migration Policy Institute. [Accessed July 26, 2015];The Limited English Proficient Population in the United States. 2015 http://www.migrationpolicy.org/article/limited-english-proficient-popula....
-
- Hampers LC, McNulty JE. Professional interpreters and bilingual physicians in a pediatric emergency department: effect on resource utilization. Arch Pediatr Adolesc Med. 2002;156(11):1108–1113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
