

Extracorporeal membrane oxygenation in severe influenza infection with respiratory failure: A systematic review and meta-analysis
- PMID: 28074789
- PMCID: PMC5290688
- DOI: 10.4103/0971-9784.197820
Extracorporeal membrane oxygenation in severe influenza infection with respiratory failure: A systematic review and meta-analysis
Abstract
Introduction: Extracorporeal membrane oxygenation (ECMO) has been extensively used for potentially reversible acute respiratory failure associated with severe influenza A (H1N1) pneumonia; however, it remains an expensive, resource-intensive therapy, with a high associated mortality. This systematic review and meta-analysis aims to summarize and pool outcomes data available in the published literature to guide clinical decision-making and further research.
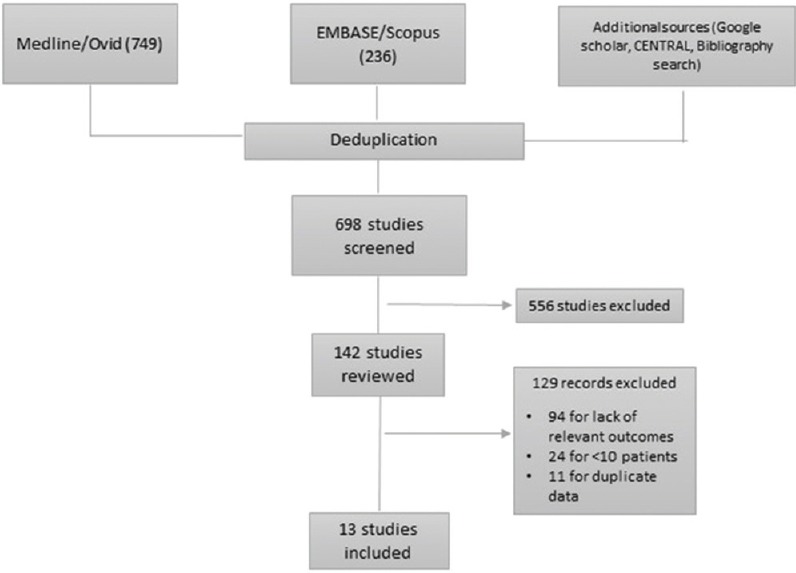
Methods: We conducted a systematic search of MEDLINE (1966 to April 15, 2015), EMBASE (1980 to April 15, 2015), CENTRAL, and Google Scholar for patients with severe H1N1 pneumonia and respiratory failure who received ECMO. The study validity was appraised by Newcastle-Ottawa Scale. The primary outcome was all-cause mortality. The secondary outcomes were duration of ECMO therapy, mechanical ventilation, and Intensive Care Unit (ICU) length of stay.
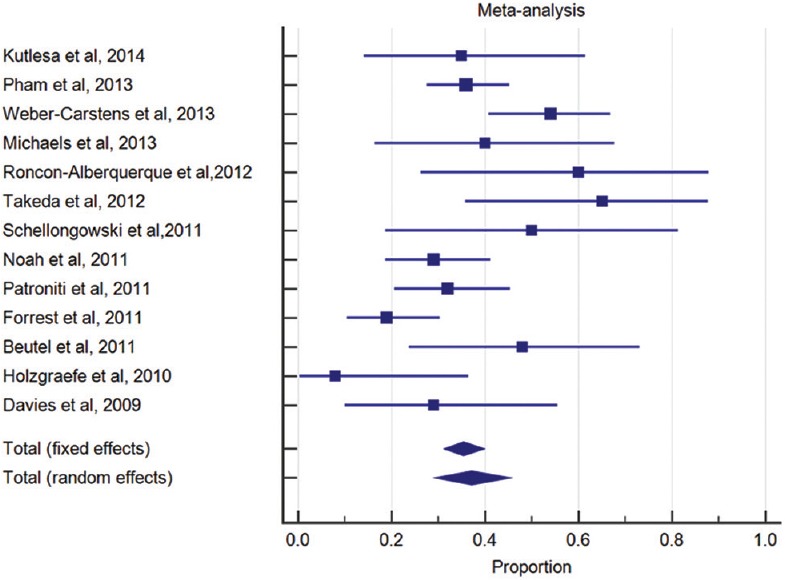
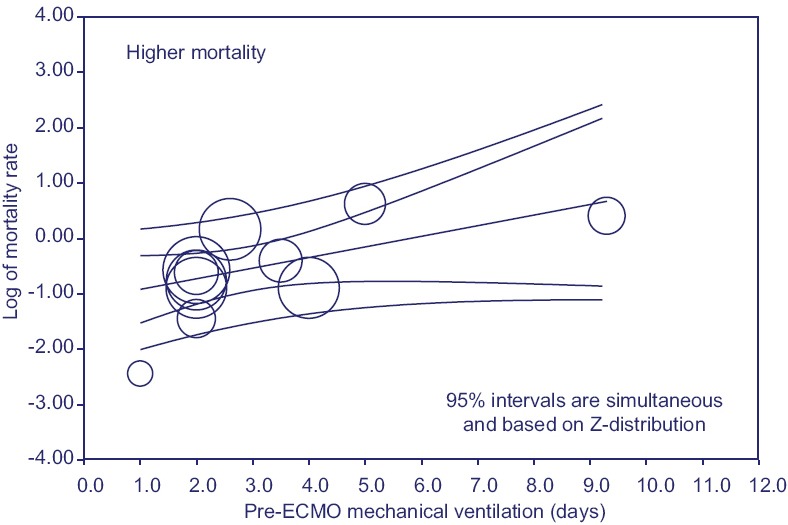
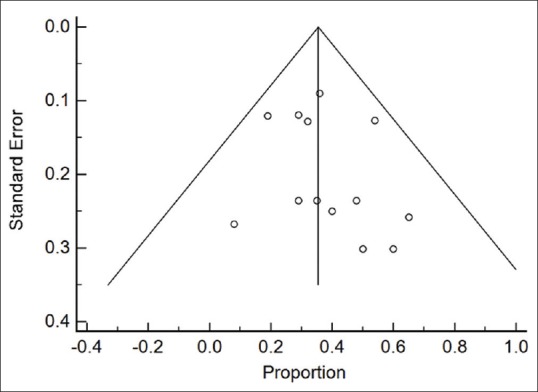
Results: Of 698 abstracts screened and 142 full-text articles reviewed, we included 13 studies with a total of 494 patients receiving ECMO in our final review and meta-analysis. The study validity was satisfactory. The overall mortality was 37.1% (95% confidence interval: 30-45%) limited by underlying heterogeneity (I2 = 65%, P value of Q statistic = 0.006). The median duration for ECMO was 10 days, mechanical ventilation was 19 days, and ICU length of stay was 33 days. Exploratory meta-regression did not identify any statistically significant moderator of mortality (P < 0.05), except for the duration of pre-ECMO mechanical ventilation in days (coefficient 0.19, standard error: 0.09, Z = 2.01, P < 0.04, R2 = 0.16). The visual inspection of funnel plots did not suggest the presence of publication bias.
Conclusions: ECMO therapy may be used as an adjunct or salvage therapy for severe H1N1 pneumonia with respiratory failure. It is associated with a prolonged duration of ventilator support, ICU length of stay, and high mortality. Initiating ECMO early once the patient has been instituted on mechanical ventilation may result in improved survival.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Vasilyev S, Schaap RN, Mortensen JD. Hospital survival rates of patients with acute respiratory failure in modern respiratory intensive care units. An international, multicenter, prospective survey. Chest. 1995;107:1083–8. - PubMed
-
- [Last accessed on 2016 Apr 28]. Available from: http://www.cdc.gov/flu/pdf/weekly/overview.pdf .
-
- Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med. 2009;151:264–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous