

Cannulation strategies in adult veno-arterial and veno-venous extracorporeal membrane oxygenation: Techniques, limitations, and special considerations
- PMID: 28074818
- PMCID: PMC5299823
- DOI: 10.4103/0971-9784.197791
Cannulation strategies in adult veno-arterial and veno-venous extracorporeal membrane oxygenation: Techniques, limitations, and special considerations
Abstract
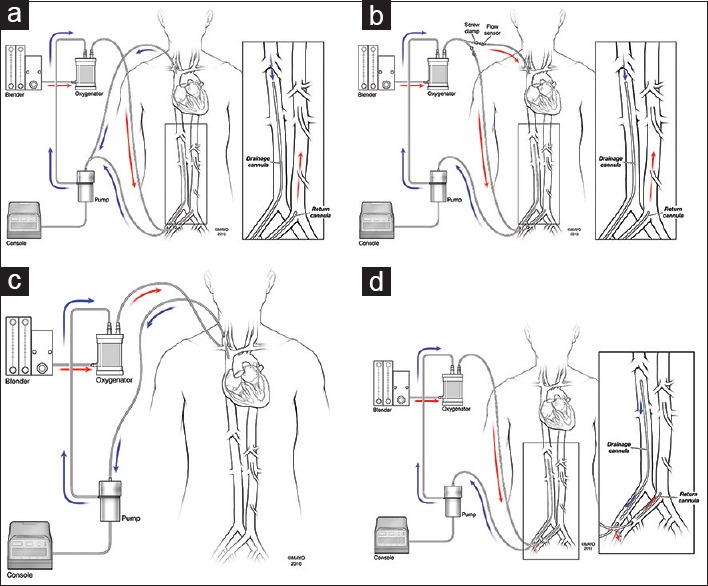
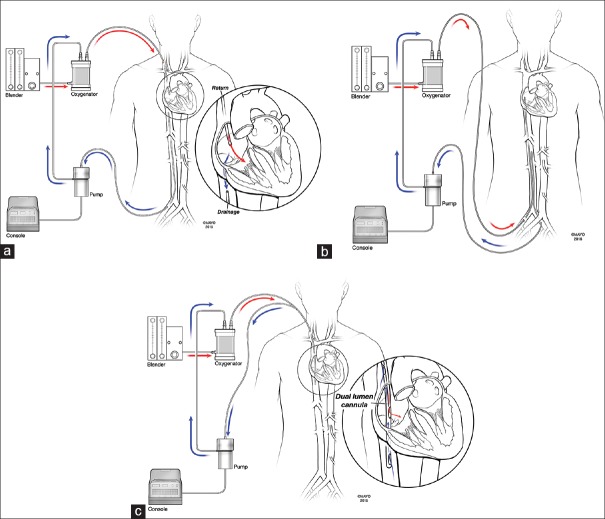
Extracorporeal membrane oxygenation (ECMO) refers to specific mechanical devices used to temporarily support the failing heart and/or lung. Technological advances as well as growing collective knowledge and experience have resulted in increased ECMO use and improved outcomes. Veno-arterial (VA) ECMO is used in selected patients with various etiologies of cardiogenic shock and entails either central or peripheral cannulation. Central cannulation is frequently used in postcardiotomy cardiogenic shock and is associated with improved venous drainage and reduced concern for upper body hypoxemia as compared to peripheral cannulation. These concerns inherent to peripheral VA ECMO may be addressed through so-called triple cannulation approaches. Veno-venous (VV) ECMO is increasingly employed in selected patients with respiratory failure refractory to more conventional measures. Newer dual lumen VV ECMO cannulas may facilitate extubation and mobilization. In summary, the pathology being addressed impacts the ECMO approach that is deployed, and each ECMO implementation has distinct virtues and drawbacks. Understanding these considerations is crucial to safe and effective ECMO use.
Figures

References
-
- Hill JD, O’Brien TG, Murray JJ, Dontigny L, Bramson ML, Osborn JJ, et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome).Use of the Bramson membrane lung. N Engl J Med. 1972;286:629–34. - PubMed
-
- Zapol WM, Snider MT, Hill JD, Fallat RJ, Bartlett RH, Edmunds LH, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA. 1979;242:2193–6. - PubMed
-
- Truby L, Mundy L, Kalesan B, Kirtane A, Colombo PC, Takeda K, et al. Contemporary outcomes of venoarterial extracorporeal membrane oxygenation for refractory cardiogenic shock at a large tertiary care center. ASAIO J. 2015;61:403–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources