

Lessons from Launching the Diabetes Prevention Program in a Large Integrated Health Care Delivery System: A Case Study
- PMID: 28075695
- PMCID: PMC5564042
- DOI: 10.1089/pop.2016.0109
Lessons from Launching the Diabetes Prevention Program in a Large Integrated Health Care Delivery System: A Case Study
Abstract
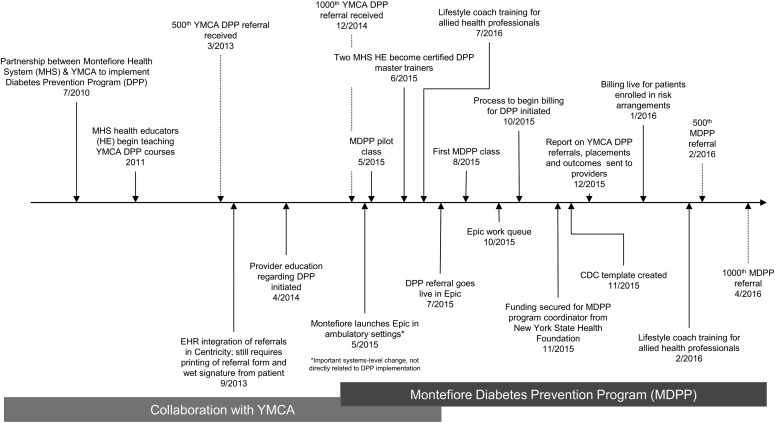
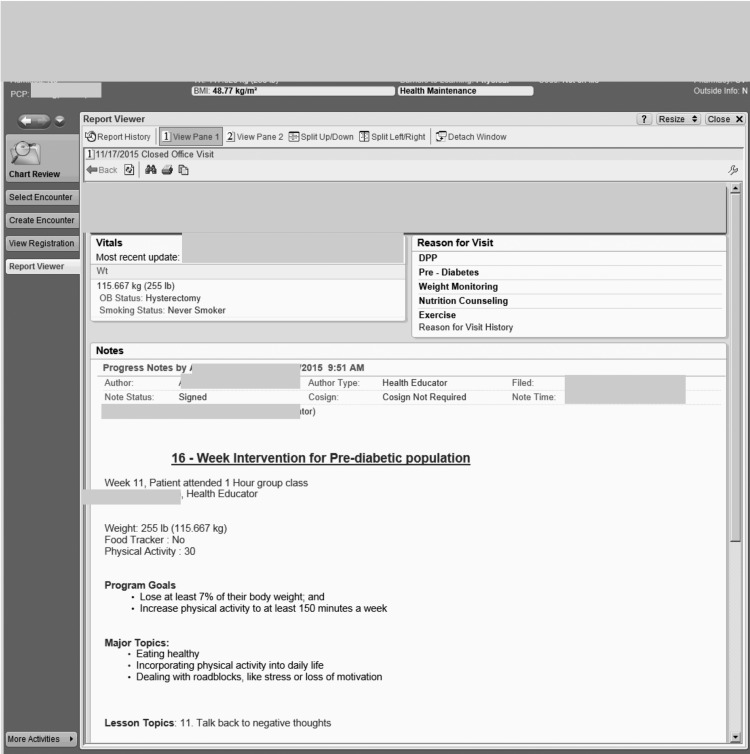
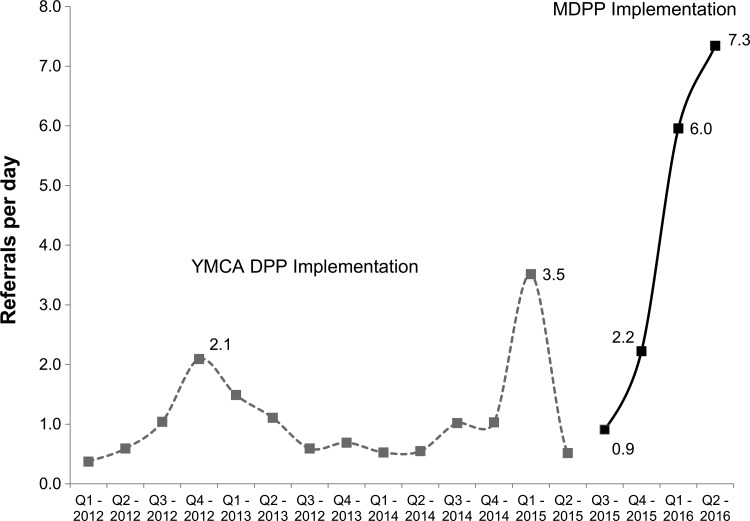
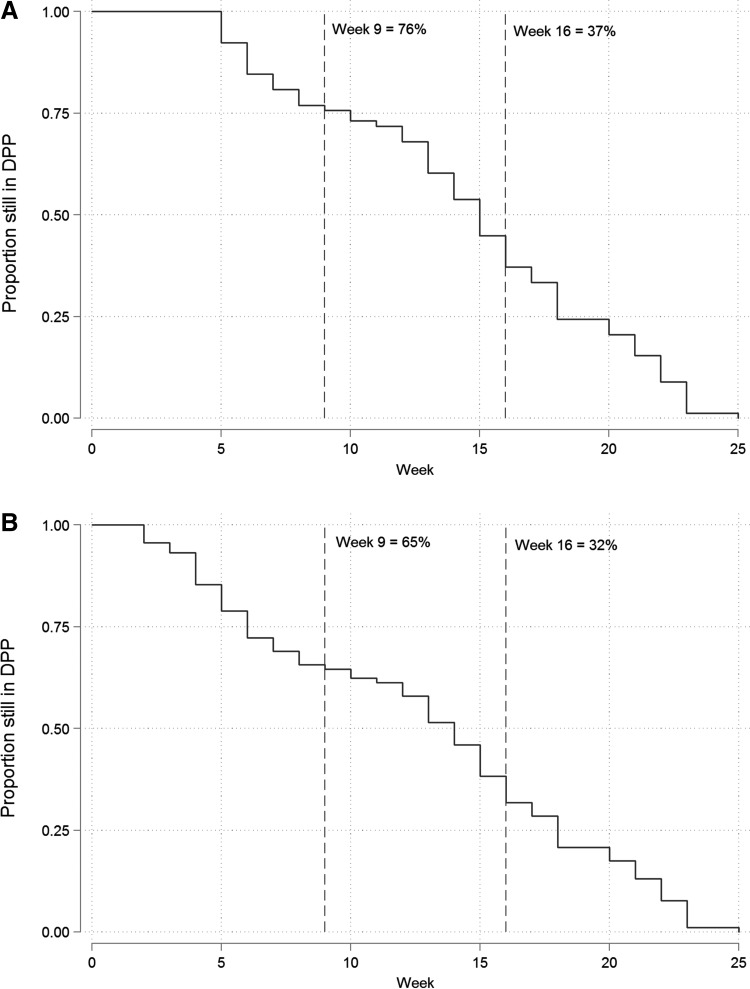
There is urgent need for health systems to prevent diabetes. To date, few health systems have implemented the evidence-based Diabetes Prevention Program (DPP), and the few that have mostly partnered with community-based organizations to implement the program. Given the recent decision by the Centers for Medicare & Medicaid Services to reimburse for diabetes prevention, there is likely much interest in how such programs can be implemented within large health systems or how community partnerships can be expanded to support DPP implementation. Beginning in 2010, Montefiore Health System (MHS), a large health care system in the Bronx, NY, partnered with the Young Men's Christian Association (YMCA) of Greater New York to deliver the YMCA's DPP. Over 4 years, 1390 referrals to YMCA's DPP were made; 287 participants attended ≥3 classes, and average weight loss was 3.4%. Because of increased patient demand and internal capacity, MHS assumed responsibility for DPP implementation in May 2015. Fully integrating the program within the health system took 5-6 months, including configuring electronic health record templates/reports, hiring a coordinator, and creating clinical referral workflows/training guides. Billing workflows were designed for risk-based contracts. In the first 11 months of implementation, 1277 referrals were made, and referrals increased over time. Twenty-four class cycles were initiated, and 282 patients began attending classes. Average weight loss among 61 graduates from the Summer/Fall 2015 wave of MDPP classes was 3.8%. Additional opportunities for expansion include training allied health staff, providing patient incentives, increasing master trainer capacity, offering DPP to employees, and securing reimbursement.
Keywords: chronic disease; diabetes; diabetes prevention.
Conflict of interest statement
Drs. Rehm, Harris-Hollingsworth, and Parsons, Ms. Marquez, and Ms. Spurrell-Huss declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for this article.
Figures
References
-
- Centers for Disease Control and Prevention. Crude and age-adjusted rates of diagnosed diabetes per 100 civilian, non-institutionalized adult population, United States, 1980–2014. www.cdc.gov/diabetes/statistics/prev/national/figageadult.htm Accessed July25, 2016
-
- Centers for Disease Control and Prevention; National Center for Health Statistics. Leading causes of death. www.cdc.gov/nchs/fastats/leading-causes-of-death.htm Accessed July24, 2016
-
- Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA 2002;287:2570–2581 - PubMed
-
- Institute for Health Metrics and Evaluation (IHME). GBD Compare. 2015. http://vizhub.healthdata.org/gbd-compare Accessed April20, 2016
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical