

A Clinical Aid for Detecting Skin Cancer: The Triage Amalgamated Dermoscopic Algorithm (TADA)
- PMID: 28076252
- PMCID: PMC5536949
- DOI: 10.3122/jabfm.2016.06.160079
A Clinical Aid for Detecting Skin Cancer: The Triage Amalgamated Dermoscopic Algorithm (TADA)
Abstract
Purpose: Family physicians (FPs) frequently evaluate skin lesions but may not have the necessary training to accurately and confidently identify lesions that require skin biopsy or specialist referral. We evaluated the diagnostic performance of a new, simplified dermoscopy algorithm for skin cancer detection.
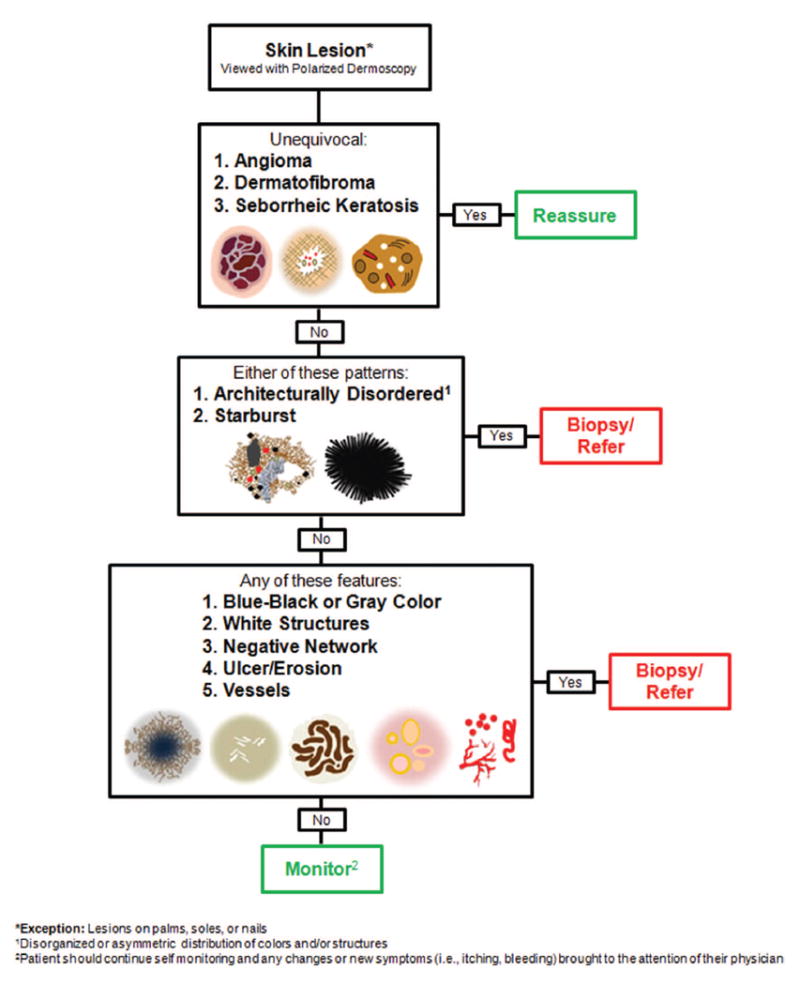
Methods: In this cross-sectional, observation study, attendees of a dermoscopy course evaluated 50 polarized dermoscopy images of skin lesions (27 malignant and 23 benign) using the Triage Amalgamated Dermoscopic Algorithm (TADA). The dermoscopic criteria of TADA include architectural disorder (ie, disorganized or asymmetric distribution of colors and/or structures), starburst pattern, blue-black or gray color, white structures, negative network, ulcer, and vessels. The study occurred after 1 day of basic dermoscopy training. Clinical information related to palpation (ie, firm, dimpling) was provided when relevant.
Results: Of 200 course attendees, 120 (60%) participated in the study. Participants included 64 (53.3%) dermatologists and 41 (34.2%) primary care physicians, 19 (46.3%) of whom were FPs. Fifty-two (43%) individuals had no previous dermoscopy training. Overall, the sensitivity and specificity of TADA for malignant skin lesions was 94.8% and 72.3%, respectively. Previous dermoscopy training and years of dermoscopy experience were not associated with diagnostic sensitivity (P = .13 and P = .05, respectively) or specificity (P = .36 and P = .21, respectively). Specialty type was not associated with sensitivity (P = .37) but dermatologists had a higher specificity than nondermatologists (79% v. 72%, P = .008).
Conclusions: After basic instruction, TADA may be a useful dermoscopy algorithm for FPs who examine skin lesions as it has a high sensitivity for detecting skin cancer.
Keywords: Algorithms; Biopsy; Cross-sectional Studies; Dermoscopy; Family; Palpation; Physicians; Referral and Consultation; Sensitivity and Specificity; Skin Neoplasms; Triage.
© Copyright 2016 by the American Board of Family Medicine.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol. 2012;166:1069–80. - PubMed
-
- McDonald CJ. American Cancer Society perspective on the American College of Preventive Medicine’s policy statements on skin cancer prevention and screening. CA Cancer J Clin. 1998;48:229–31. - PubMed
-
- Kimball AB, Resneck JS., Jr The US dermatology workforce: A specialty remains in shortage. J Am Acad Dermatol. 2008;59:741–5. - PubMed
-
- Uhlenhake E, Brodell R, Mostow E. The dermatology work force: A focus on urban versus rural wait times. J Am Acad Dermatol. 2009;61:17–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous