

Anti-Epileptic Drug Combination Efficacy in an In Vitro Seizure Model - Phenytoin and Valproate, Lamotrigine and Valproate
- PMID: 28076384
- PMCID: PMC5226812
- DOI: 10.1371/journal.pone.0169974
Anti-Epileptic Drug Combination Efficacy in an In Vitro Seizure Model - Phenytoin and Valproate, Lamotrigine and Valproate
Abstract
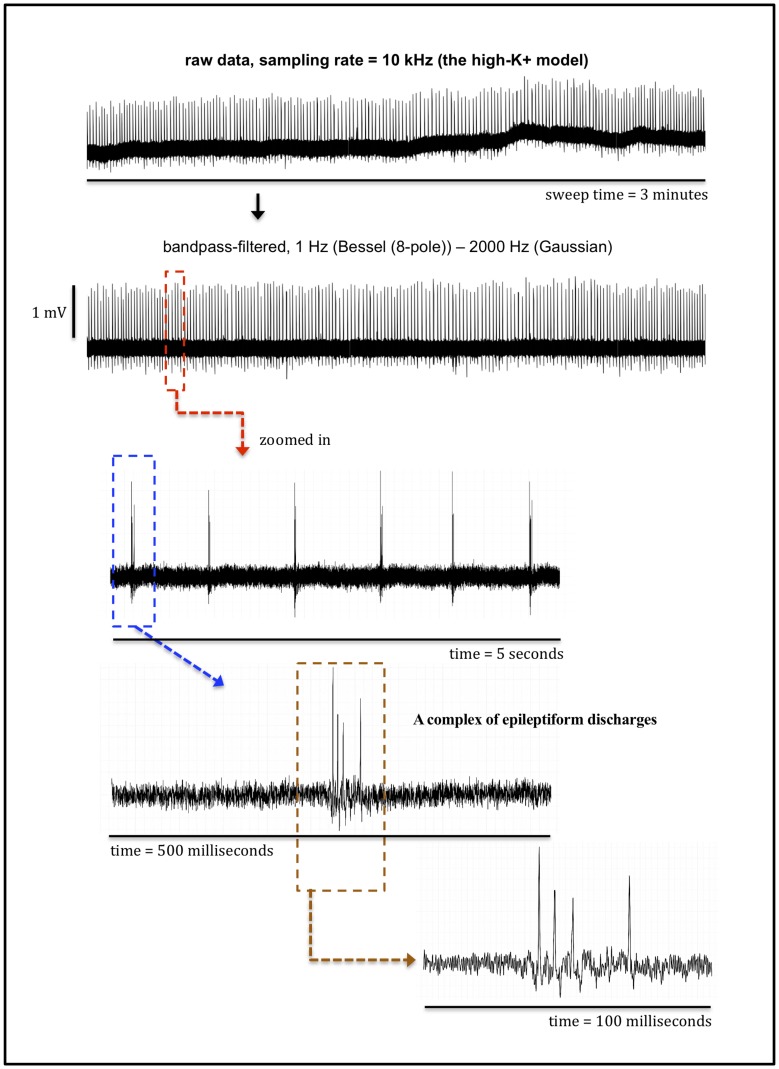
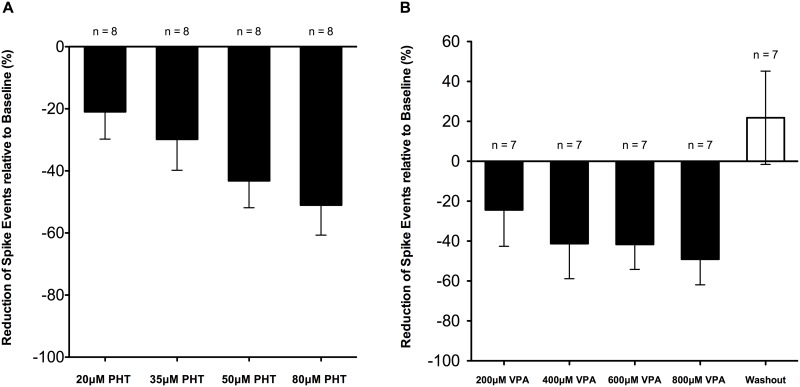
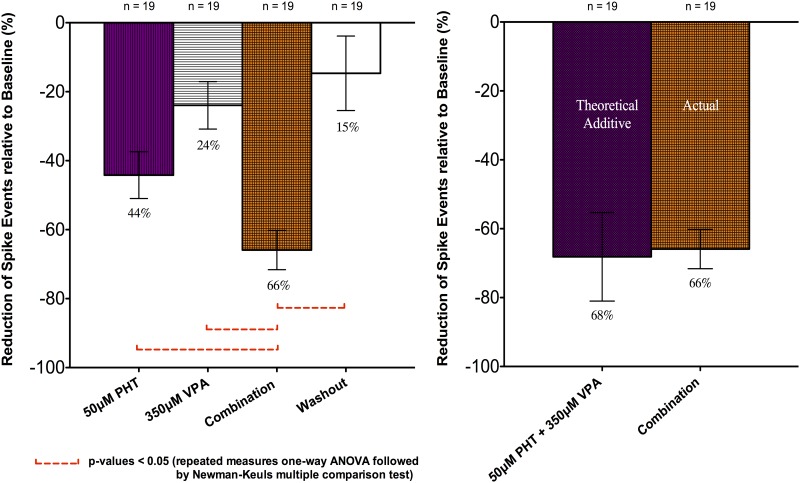
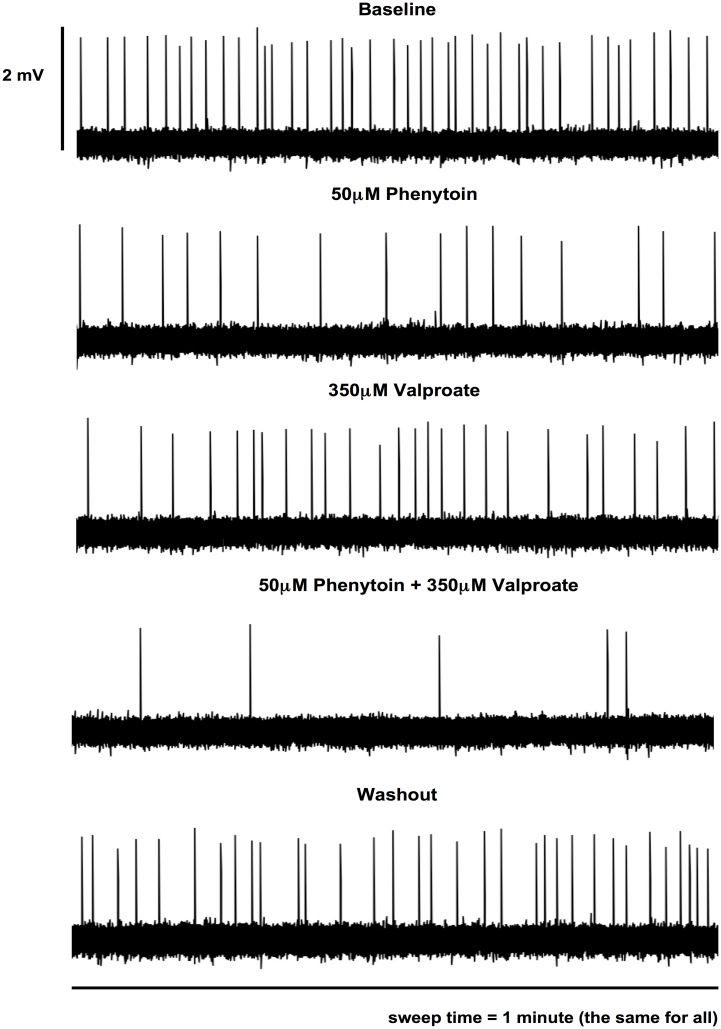
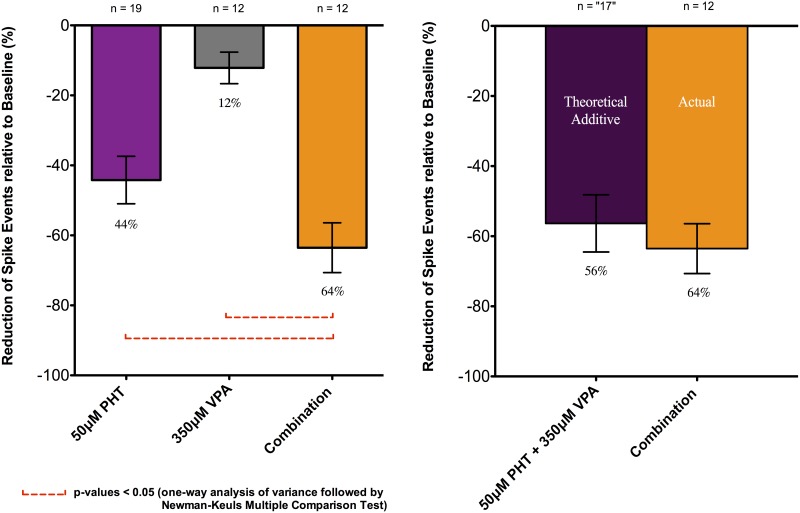
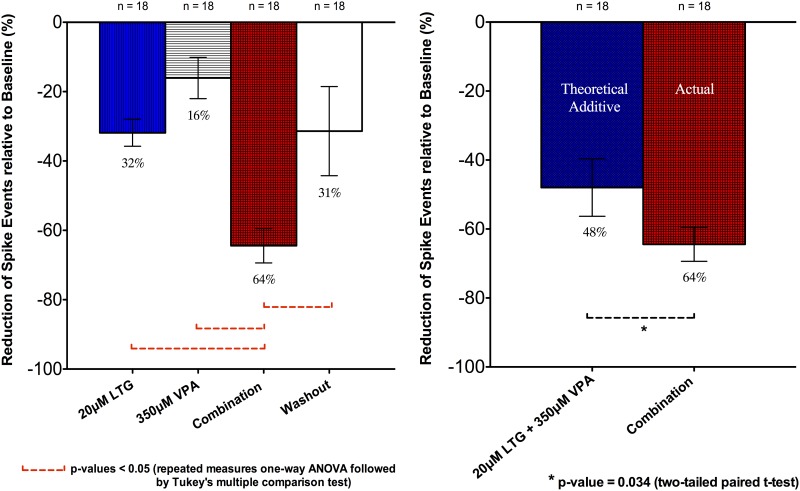
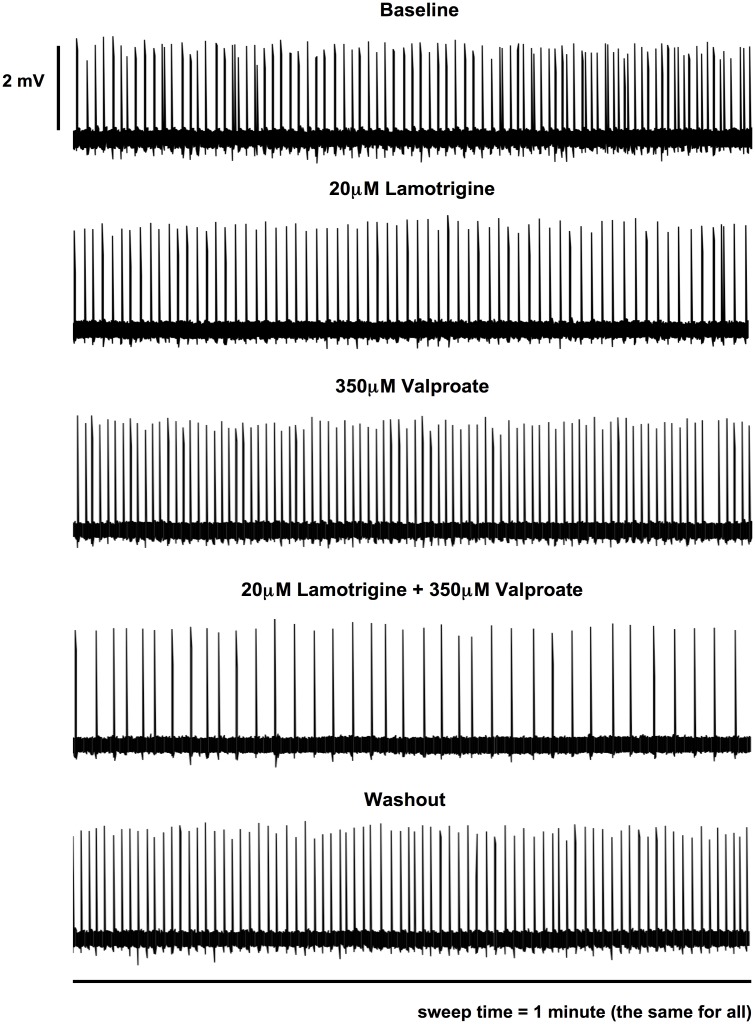
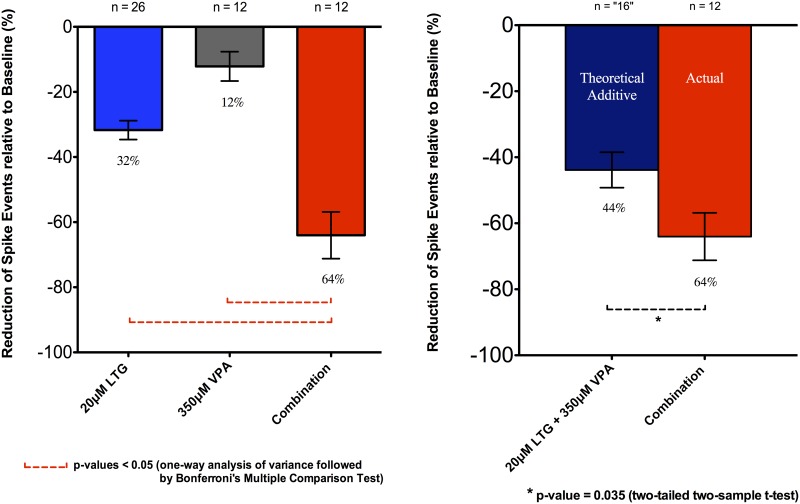
In this study, we investigated the relative efficacy of different classes of commonly used anti-epileptic drugs (AEDs) with different mechanisms of action, individually and in combination, to suppress epileptiform discharges in an in vitro model. Extracellular field potential were recorded in 450 μm thick transverse hippocampal slices prepared from juvenile Wistar rats, in which "epileptiform discharges" (ED's) were produced with a high-K+ (8.5 mM) bicarbonate-buffered saline solution. Single and dual recordings in stratum pyramidale of CA1 and CA3 regions were performed with 3-5 MΩ glass microelectrodes. All drugs-lamotrigine (LTG), phenytoin (PHT) and valproate (VPA)-were applied to the slice by superfusion at a rate of 2 ml/min at 32°C. Effects upon frequency of ED's were assessed for LTG, PHT and VPA applied at different concentrations, in isolation and in combination. We demonstrated that high-K+ induced ED frequency was reversibly reduced by LTG, PHT and VPA, at concentrations corresponding to human therapeutic blood plasma concentrations. With a protocol using several applications of drugs to the same slice, PHT and VPA in combination displayed additivity of effect with 50μM PHT and 350μM VPA reducing SLD frequency by 44% and 24% individually (n = 19), and together reducing SLD frequency by 66% (n = 19). 20μM LTG reduced SLD frequency by 32% and 350μM VPA by 16% (n = 18). However, in combination there was a supra-linear suppression of ED's of 64% (n = 18). In another independent set of experiments, similar results of drug combination responses were also found. In conclusion, a combination of conventional AEDs with different mechanisms of action, PHT and VPA, displayed linear additivity of effect on epileptiform activity. More intriguingly, a combination of LTG and VPA considered particularly efficacious clinically showed a supra-additive suppression of ED's. This approach may be useful as an in vitro platform for assessing drug combination efficacy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
