

Diffusion of Evidence-based Intensive Care Unit Organizational Practices. A State-Wide Analysis
- PMID: 28076685
- PMCID: PMC5427731
- DOI: 10.1513/AnnalsATS.201607-579OC
Diffusion of Evidence-based Intensive Care Unit Organizational Practices. A State-Wide Analysis
Abstract
Rationale: Several intensive care unit (ICU) organizational practices have been associated with improved patient outcomes. However, the uptake of these evidence-based practices is unknown.
Objectives: To assess diffusion of ICU organizational practices across the state of Pennsylvania.
Methods: We conducted two web-based, cross-sectional surveys of ICU organizational practices in Pennsylvania acute care hospitals, in 2005 (chief nursing officer respondents) and 2014 (ICU nurse manager respondents).
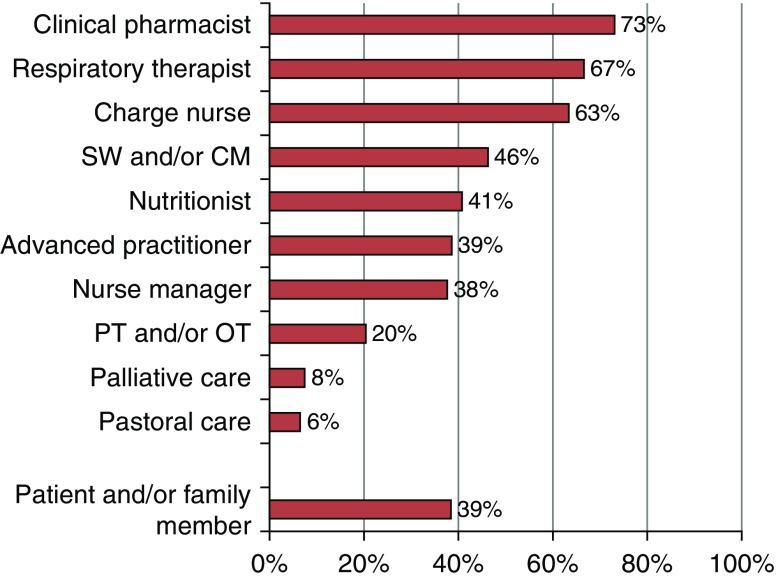
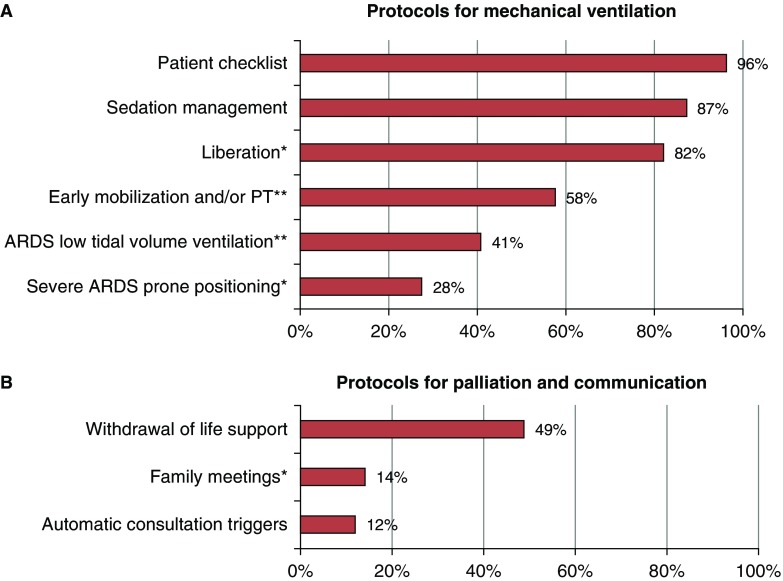
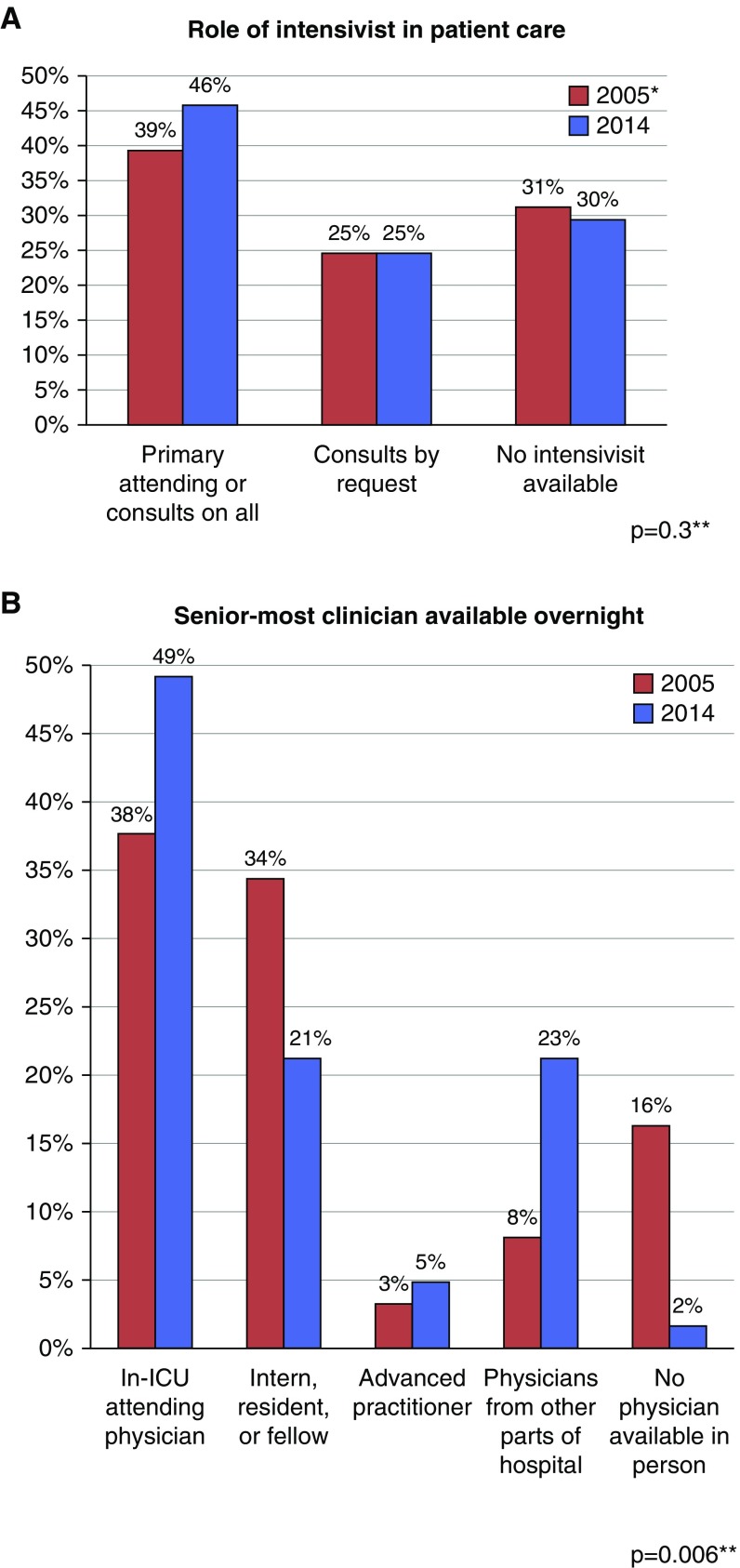
Measurements and main results: Of 223 eligible respondents, nurse managers from 136 (61%) medical, surgical, mixed medical-surgical, cardiac, and specialty ICUs in 98 hospitals completed the 2014 survey, compared with 124 of 164 (76%) chief nursing officers in the 2005 survey. In 2014, daytime physician staffing models varied widely, with 23 of 136 (17%) using closed models and 33 (24%) offering no intensivist staffing. Nighttime intensivist staffing was used in 37 (27%) ICUs, 38 (28%) used nonintensivist attending staffing, and 24 (18%) had no nighttime attending physicians. Daily multidisciplinary rounds occurred in 93 (68%) ICUs. Regular participants included clinical pharmacists in 68 of 93 (73%) ICUs, respiratory therapists in 62 (67%), and advanced practitioners in 37 (39%). Patients and family members participated in rounds in 36 (39%) ICUs. Clinical protocols or checklists for mechanically ventilated patients were available in 128 of 133 (96%) ICUs, low tidal volume ventilation for acute respiratory distress syndrome in 54 of 132 (41%) ICUs, prone positioning for severe acute respiratory distress syndrome in 37 of 134 (28%) ICUs, and family meetings in 19 of 134 (14%) ICUs. Among 61 ICUs that responded to both surveys, there was a significant increase in the proportion of ICUs using nighttime in-ICU attending physicians (23 [38%] in 2005 vs. 30 [49%] in 2014; P = 0.006).
Conclusions: The diffusion of evidence-based ICU organizational practices has been variable across the state of Pennsylvania. Only half of Pennsylvania ICUs have intensivists dedicated to the ICU. Variable numbers use clinical protocols for life-saving therapies, and few use structured family engagement strategies. In contrast, the diffusion of non-evidence-based practices, including overnight ICU attending physician staffing, is increasing. Future research should focus on promoting implementation of organizational evidence to promote high-quality ICU care.
Keywords: clinical protocols; intensive care units; multidisciplinary communication; patient-centered care; personnel staffing.
Figures
References
-
- Checkley W, Martin GS, Brown SM, Chang SY, Dabbagh O, Fremont RD, Girard TD, Rice TW, Howell MD, Johnson SB, et al. United States Critical Illness and Injury Trials Group Critical Illness Outcomes Study Investigators. Structure, process, and annual ICU mortality across 69 centers: United States Critical Illness and Injury Trials Group Critical Illness Outcomes Study. Crit Care Med. 2014;42:344–356. - PMC - PubMed
-
- Boev C, Xue Y, Ingersoll GL. Nursing job satisfaction, certification and healthcare-associated infections in critical care. Intensive Crit Care Nurs. 2015;31:276–284. - PubMed
-
- Boyle DK, Cramer E, Potter C, Gatua MW, Stobinski JX. The relationship between direct-care RN specialty certification and surgical patient outcomes. AORN J. 2014;100:511–528. - PubMed
-
- Sakr Y, Moreira CL, Rhodes A, Ferguson ND, Kleinpell R, Pickkers P, Kuiper MA, Lipman J, Vincent JL Extended Prevalence of Infection in Intensive Care Study Investigators. The impact of hospital and ICU organizational factors on outcome in critically ill patients: results from the Extended Prevalence of Infection in Intensive Care study. Crit Care Med. 2015;43:519–526. - PubMed
-
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA. 2002;288:2151–2162. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
