

Clonal evolution in therapy-related neoplasms
- PMID: 28076841
- PMCID: PMC5355323
- DOI: 10.18632/oncotarget.14509
Clonal evolution in therapy-related neoplasms
Abstract
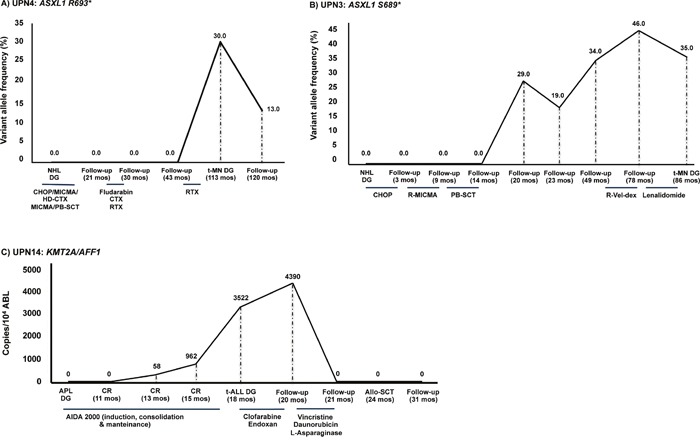
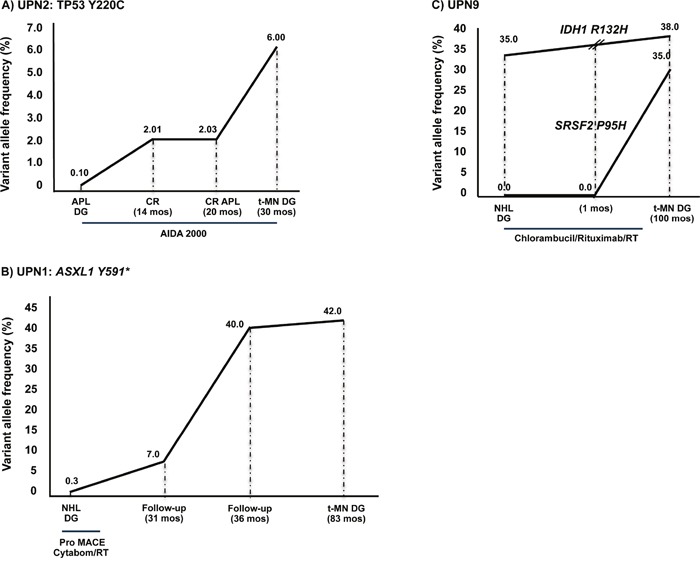
Therapy-related myeloid neoplasms (t-MN) may occur as a late effect of cytotoxic therapy for a primary malignancy or autoimmune diseases in susceptible individuals. We studied the development of somatic mutations in t-MN, using a collection of follow-up samples from 14 patients with a primary hematologic malignancy, who developed a secondary leukemia (13 t-MN and 1 t-acute lymphoblastic leukemia), at a median latency of 73 months (range 18-108) from primary cancer diagnosis.Using Sanger and next generation sequencing (NGS) approaches we identified 8 mutations (IDH1 R132H, ASXL1 Y591*, ASXL1 S689*, ASXL1 R693*, SRSF2 P95H, SF3B1 K700E, SETBP1 G870R and TP53 Y220C) in seven of thirteen t-MN patients (54%), whereas the t-ALL patient had a t(4,11) translocation, resulting in the KMT2A/AFF1 fusion gene. These mutations were then tracked backwards in marrow samples preceding secondary leukemia occurrence, using pyrosequencing and a NGS protocol that allows the detection of low variant allele frequencies (≥0.1%).Somatic mutations were detectable in the BM harvested at the primary diagnosis, prior to any cytotoxic treatment in three patients, while they were not detectable and apparently acquired by the t-MN clone in five patients.These data show that clonal evolution in t-MN is heterogeneous, with some somatic mutations preceding cytotoxic treatment and possibly favoring leukemic development.
Keywords: NGS; clonal evolution; mutation; therapy-related neoplasms.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
-
- Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM, Hellström-Lindberg E, Tefferi A, Bloomfield CD. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114:937–51. doi: 10.1182/blood-2009-03-209262. - DOI - PubMed
-
- Fianchi L, Pagano L, Piciocchi A, Candoni A, Gaidano G, Breccia M, Criscuolo M, Specchia G, E Maria Pogliani, Maurillo L, Aloe-Spiriti MA, Mecucci C, Niscola P, et al. Characteristics and outcome of therapy-related myeloid neoplasms: Report from the Italian network on secondary leukemias. Am J Hematol. 2015;90:E80–5. doi: 10.1002/ajh.23966. - DOI - PubMed
-
- Pagano L, Pulsoni A, Tosti ME, Annino L, Mele A, Camera A, Martino B, Guglielmi C, Cerri R, Di Bona E, Invernizzi R, Castagnola C, Bassan R, et al. Acute lymphoblastic leukaemia occurring as second malignancy: report of the GIMEMA archive of adult acute leukaemia. Gruppo Italiano Malattie Ematologiche Maligne dell'Adulto. Br J Haematol. 1999;106:1037–40. - PubMed
-
- Pedersen-Bjergaard J. Acute lymphoid leukemia with t(4;11)(q21;q23) following chemo-therapy with cytostatic agents targeting at DNA-topoisomerase II. Leuk Res. 1992;16:733–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
