

Treatment planning comparison of IMPT, VMAT and 4π radiotherapy for prostate cases
- PMID: 28077128
- PMCID: PMC5225526
- DOI: 10.1186/s13014-016-0761-0
Treatment planning comparison of IMPT, VMAT and 4π radiotherapy for prostate cases
Abstract
Background: Intensity-modulated proton therapy (IMPT), non-coplanar 4π intensity-modulated radiation therapy (IMRT), and volumetric-modulated arc therapy (VMAT) represent the most advanced treatment methods based on heavy ion and X-rays, respectively. Here we compare their performance for prostate cancer treatment.
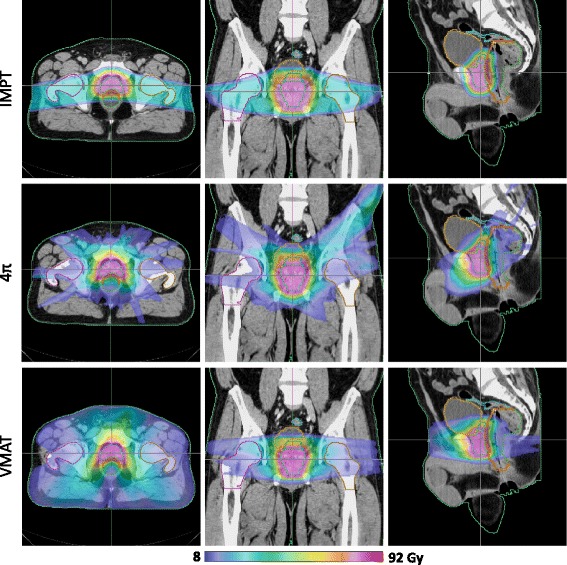
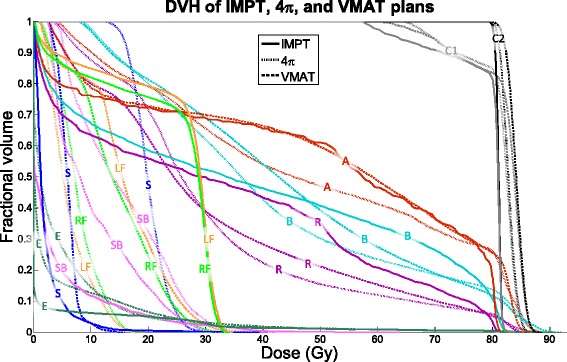
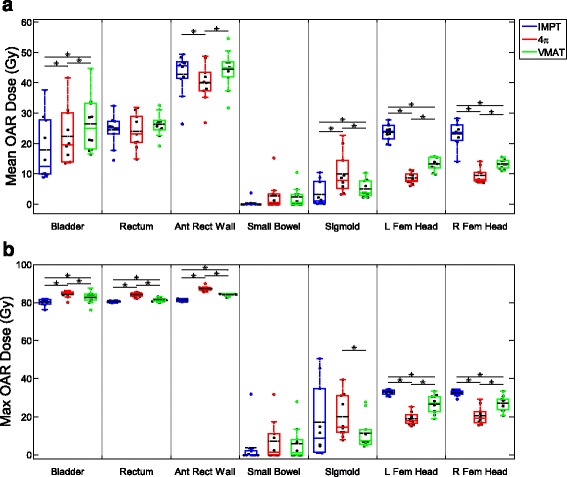
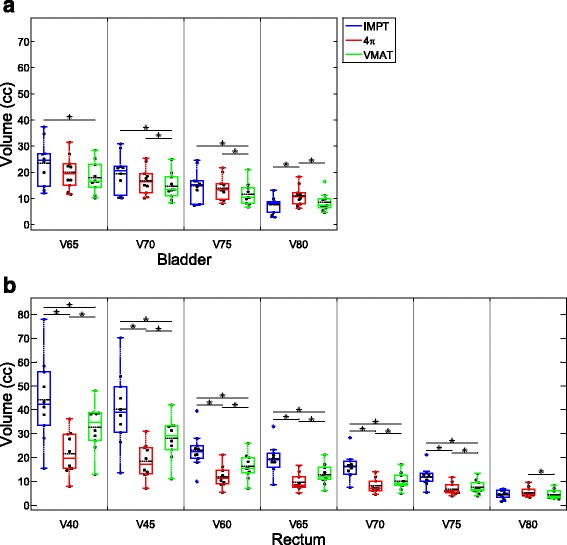
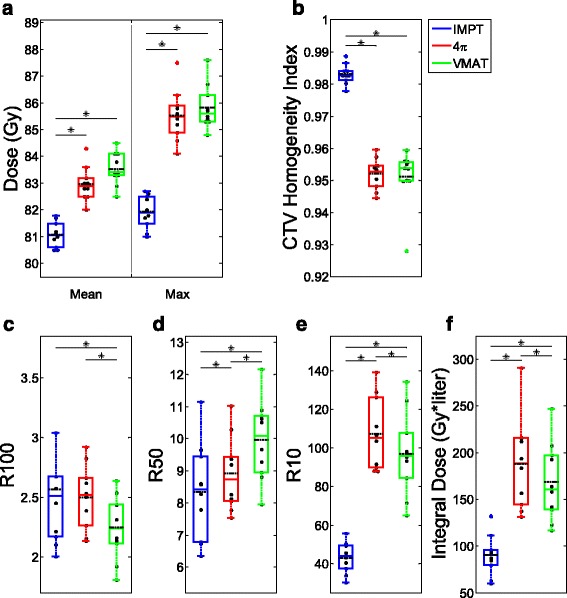
Methods: Ten prostate patients were planned using IMPT with robustness optimization, VMAT, and 4π to an initial dose of 54 Gy to a clinical target volume (CTV) that encompassed the prostate and seminal vesicles, then a boost prescription dose of 25.2 Gy to the prostate for a total dose of 79.2 Gy. The IMPT plans utilized two coplanar, oblique scanning beams 10° posterior of the lateral beam positions. Range uncertainties were taken into consideration in the IMPT plans. VMAT plans used two full, coplanar arcs to ensure sufficient PTV coverage. 4π plans were created by inversely selecting and optimizing 30 beams from 1162 candidate non-coplanar beams using a greedy column generation algorithm. CTV doses, bladder and rectum dose volumes (V40, V45, V60, V65, V70, V75, and V80), R100, R50, R10, and CTV homogeneity index (D95/D5) were evaluated.
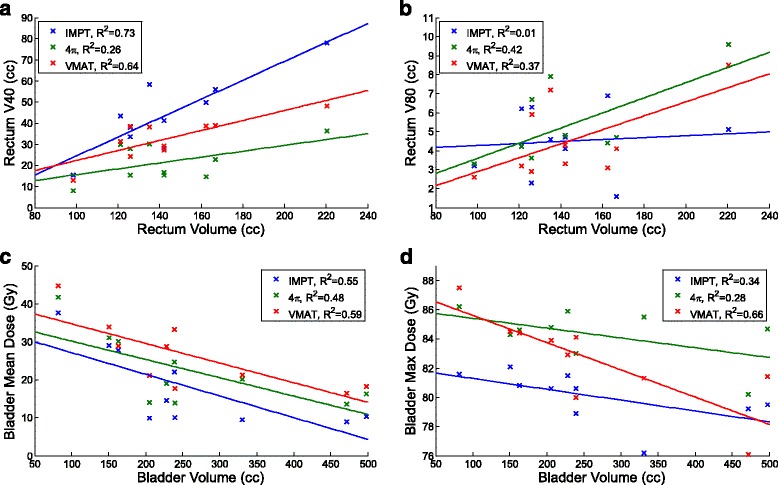
Results: Compared to IMPT, 4π resulted in lower anterior rectal wall mean dose as well as lower rectum V40, V45, V60, V65, V70, and V75. Due to the opposing beam arrangement, IMPT resulted in significantly (p < 0.05) greater femoral head doses. However, IMPT plans had significantly lower bladder, rectum, and anterior rectal wall max dose. IMPT doses were also significantly more homogeneous than 4π and VMAT doses.
Conclusion: Compared to the VMAT and 4π plans, IMPT treatment plans are superior in CTV homogeneity and maximum point organ-at-risk (OAR) doses with the exception of femur heads. IMPT is inferior in rectum and bladder volumes receiving intermediate to high doses, particularly to the 4π plans, but significantly reduced low dose spillage and integral dose, which are correlated to secondary cancer for patients with expected long survival. The dosimetric benefits of 4π plans over VMAT are consistent with the previous publication.
Keywords: 4π radiotherapy; Intensity modulated proton therapy; Prostate cancer; Volumetric modulated arc therapy.
Figures
Comment in
-
In regard to "Tran A, Zhang J, Woods K, Yu V, Nguyen D, Gustafson G, Rosen L, Sheng K. Treatment planning comparison of IMPT, VMAT and 4π radiotherapy for prostate cases. Radiation oncology. 2017 Jan 11; 12(1):10".Radiat Oncol. 2018 Apr 12;13(1):63. doi: 10.1186/s13014-018-1009-y. Radiat Oncol. 2018. PMID: 29650027 Free PMC article.
References
-
- American Cancer Society. Cancer Facts & Figures 2015. Atlanta: American Cancer Society; 2015. http://www.cancer.org/acs/groups/content/@editorial/documents/document/a....
-
- Pederson AW, Fricano J, Correa D, Pelizzari CA, Liauw SL. Late toxicity after intensity-modulated radiation therapy for localized prostate cancer: an exploration of dose-volume histogram parameters to limit genitourinary and gastrointestinal toxicity. Int J Radiat Oncol Biol Phys. 2012;82:235–41. doi: 10.1016/j.ijrobp.2010.09.058. - DOI - PubMed
-
- Albertini F, Gaignat S, Bosshardt M, Lomax AJ. Planning and Optimizing Treatment Plans for Actively Scanned Proton Therapy. In: Censor Y, Jiang M, Wang G, editors. Biomedical Mathematics: Promising Directions in Imaging, Therapy Planning, and Inverse Problems (ed 1). Madison: Medical Physics Pub Corp; 2009. pp. 1–18.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
