

Evidence for overuse of medical services around the world
- PMID: 28077234
- PMCID: PMC5708862
- DOI: 10.1016/S0140-6736(16)32585-5
Evidence for overuse of medical services around the world
Erratum in
-
Department of Error.Lancet. 2022 Mar 5;399(10328):908. doi: 10.1016/S0140-6736(22)00374-9. Lancet. 2022. PMID: 35248184 No abstract available.
Abstract
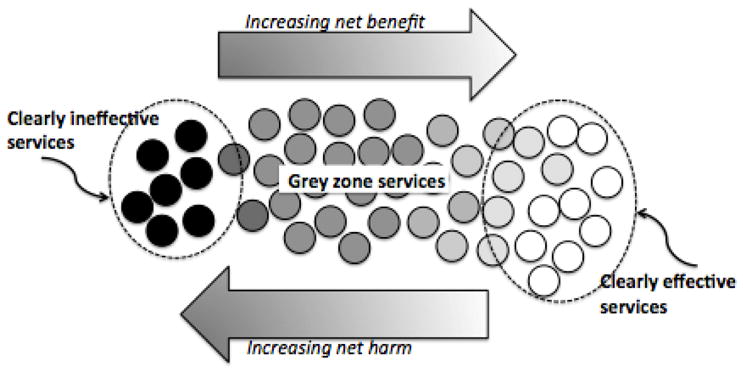
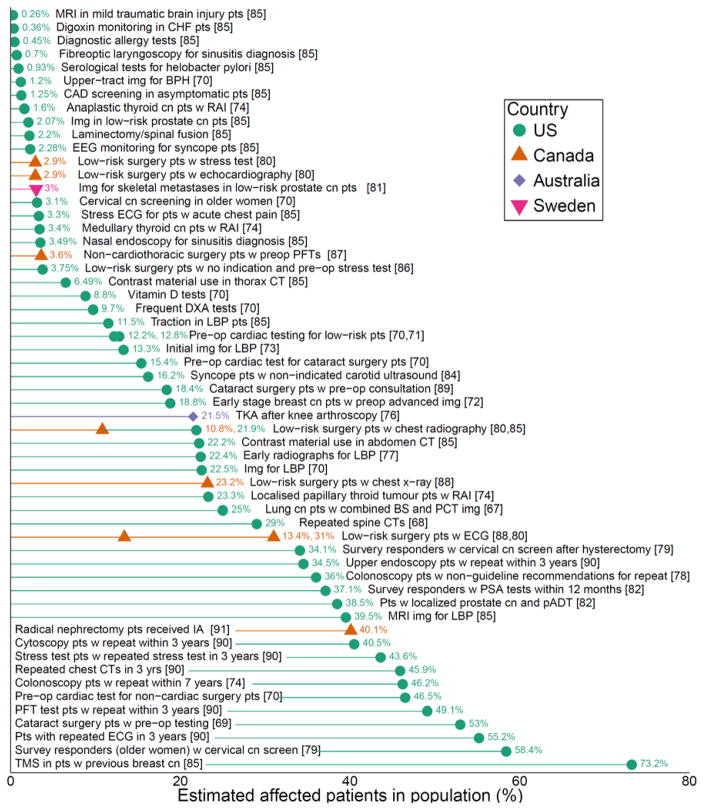
Overuse, which is defined as the provision of medical services that are more likely to cause harm than good, is a pervasive problem. Direct measurement of overuse through documentation of delivery of inappropriate services is challenging given the difficulty of defining appropriate care for patients with individual preferences and needs; overuse can also be measured indirectly through examination of unwarranted geographical variations in prevalence of procedures and care intensity. Despite the challenges, the high prevalence of overuse is well documented in high-income countries across a wide range of services and is increasingly recognised in low-income countries. Overuse of unneeded services can harm patients physically and psychologically, and can harm health systems by wasting resources and deflecting investments in both public health and social spending, which is known to contribute to health. Although harms from overuse have not been well quantified and trends have not been well described, overuse is likely to be increasing worldwide.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Interests
AGE receives salary support as the HCF Research Foundation Principal Research Fellow, and holds research grants from The Commonwealth Fund and Australia’s National Health and Medical Research Council (ID 1109626 and 1104136). AGE receives consulting/sitting fees from Cancer Australia, the Capital Markets Cooperative Research Centre-Health Quality Program, NPS MedicineWise (facilitator of Choosing Wisely Australia), The Royal Australasian College of Physicians (facilitator of the EVOLVE program) and the Australian Commission on Safety and Quality in Health Care. JD reports grants from NHMRC. VS and SB receive support from a grant from the Robert Wood Johnson Foundation. DK was supported by a Cancer Center Support Grant from the National Cancer Institute to Memorial Sloan Kettering Cancer Center (award number P30 CA008748). KC, KChalmers, SN, DS, PG, and IH report nothing to disclose.
Figures
Comment in
-
Avoiding overuse-the next quality frontier.Lancet. 2017 Jul 8;390(10090):102-104. doi: 10.1016/S0140-6736(16)32570-3. Epub 2017 Jan 9. Lancet. 2017. PMID: 28077229 No abstract available.
-
Addressing overuse and underuse around the world.Lancet. 2017 Jul 8;390(10090):105-107. doi: 10.1016/S0140-6736(16)32573-9. Epub 2017 Jan 9. Lancet. 2017. PMID: 28077230 No abstract available.
-
The future of radiology: adding value to clinical care.Lancet. 2018 Aug 11;392(10146):472-473. doi: 10.1016/S0140-6736(18)31193-0. Epub 2018 Aug 9. Lancet. 2018. PMID: 30129453 No abstract available.
References
-
- Chassin MR, Galvin RW. The urgent need to improve health care quality. Institute of Medicine National Roundtable on Health Care Quality. JAMA : the journal of the American Medical Association. 1998;280(11):1000–5. - PubMed
-
- Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA : the journal of the American Medical Association. 2012;307(14):1513–6. - PubMed
-
- Wennberg JE, Fisher ES, Skinner JS. Geography and the debate over Medicare reform. Health affairs. 2002;(Suppl Web Exclusives):W96–114. - PubMed
-
- Chalmers K, Elshaug AG. An inventory of low-value care measured from two perspectives: Inappropriate care versus wasted services. 2016 Unpulbished Manuscript Under Review.
-
- Elshaug AG, Watt AM, Mundy L, Willis CD. Over 150 potentially low-value health care practices: an Australian study. Med J Aust. 2012;197(10):556–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
