

Have health inequalities changed during childhood in the New Labour generation? Findings from the UK Millennium Cohort Study
- PMID: 28077409
- PMCID: PMC5253527
- DOI: 10.1136/bmjopen-2016-012868
Have health inequalities changed during childhood in the New Labour generation? Findings from the UK Millennium Cohort Study
Abstract
Objectives: To examine how population-level socioeconomic health inequalities developed during childhood, for children born at the turn of the 21st century and who grew up with major initiatives to tackle health inequalities (under the New Labour Government).
Setting: The UK.
Participants: Singleton children in the Millennium Cohort Study at ages 3 (n=15 381), 5 (n=15 041), 7 (n=13 681) and 11 (n=13 112) years.
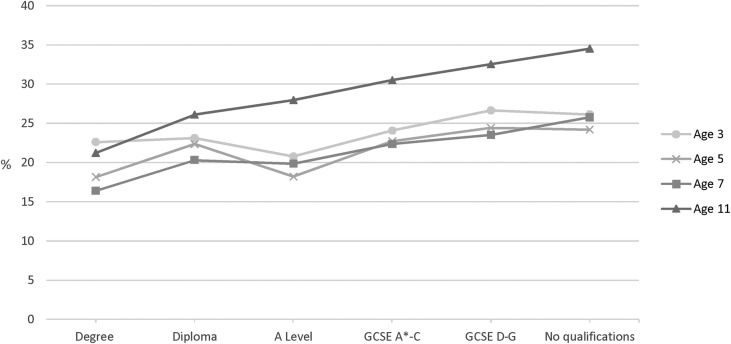
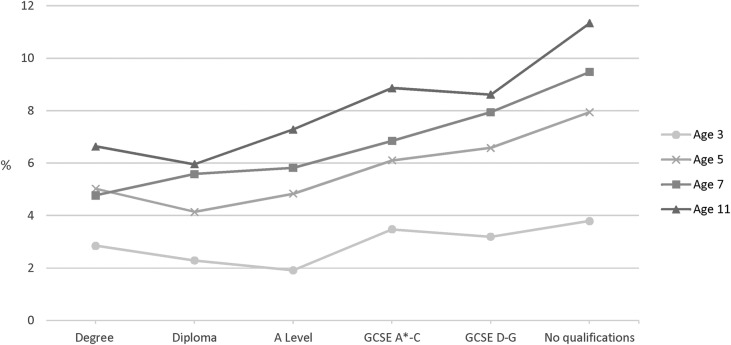
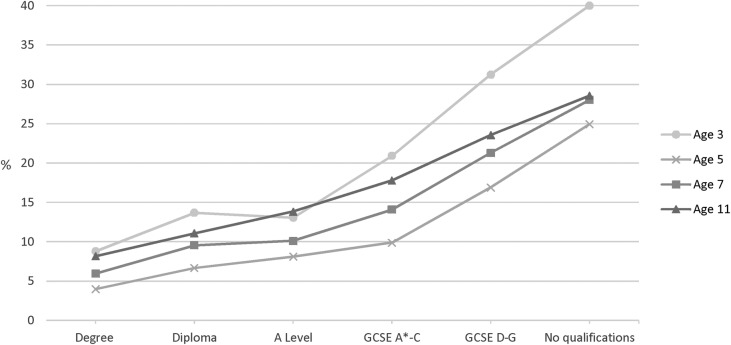
Primary outcomes: Relative (prevalence ratios (PR)) and absolute health inequalities (prevalence differences (PD)) were estimated in longitudinal models by socioeconomic circumstances (SEC; using highest maternal academic attainment, ranging from 'no academic qualifications' to 'degree' (baseline)). Three health outcomes were examined: overweight (including obesity), limiting long-standing illness (LLSI), and socio-emotional difficulties (SED).
Results: Relative and absolute inequalities in overweight, across the social gradient, emerged by age 5 and increased with age. By age 11, children with mothers who had no academic qualifications were considerably more likely to be overweight as compared with those with degree-educated mothers (PR=1.6 (95% CI 1.4 to 1.8), PD=12.9% (9.1% to 16.8%)). For LLSI, inequalities emerged by age 7 and remained at 11, but only for children whose mothers had no academic qualifications (PR=1.7 (1.3 to 2.3), PD=4.8% (2% to 7.5%)). Inequalities in SED (observed across the social gradient and at all ages) declined between 3 and 11, although remained large at 11 (eg, PR=2.4 (1.9 to 2.9), PD=13.4% (10.2% to 16.7%) comparing children whose mothers had no academic qualifications with those of degree-educated mothers).
Conclusions: Although health inequalities have been well documented in cross-sectional and trend data in the UK, it is less clear how they develop during childhood. We found that relative and absolute health inequalities persisted, and in some cases widened, for a cohort of children born at the turn of the century. Further research examining and comparing the pathways through which SECs influence health may further our understanding of how inequalities could be prevented in future generations of children.
Keywords: CHILD HEALTH; COHORT; INEQUALITIES; LIFECOURSE EPIDEMIOLOGY; POLICY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes 2011;35:891–8. - PubMed
-
- Williams L. Annual Report of the Chief Medical Officer 2012. Our Children Deserve Better: Prevention Pays. London: Department of Health, 2013.
-
- Dinsdale H, Hancock C, Rutter H. National Child Measurement Programme. Changes in children's BMI between 2006/7 and 2012/13. London: Public Health England, 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials