

Dystonia treatment: Patterns of medication use in an international cohort
- PMID: 28077492
- PMCID: PMC5304465
- DOI: 10.1212/WNL.0000000000003596
Dystonia treatment: Patterns of medication use in an international cohort
Abstract
Objective: To determine the frequency of medication use in patients with dystonia enrolled in an international biorepository study.
Methods: In a cross-sectional analysis, we included 2,026 participants enrolled at 37 sites in the United States, Canada, Europe, and Australia through Project 1 of the Dystonia Coalition, an international biorepository study. The primary aim was to assess the frequency of medication classes recommended for treating patients with dystonia, and the secondary aim was to compare characteristics (disease type, age, sex, duration of disease, comorbid conditions, severity).
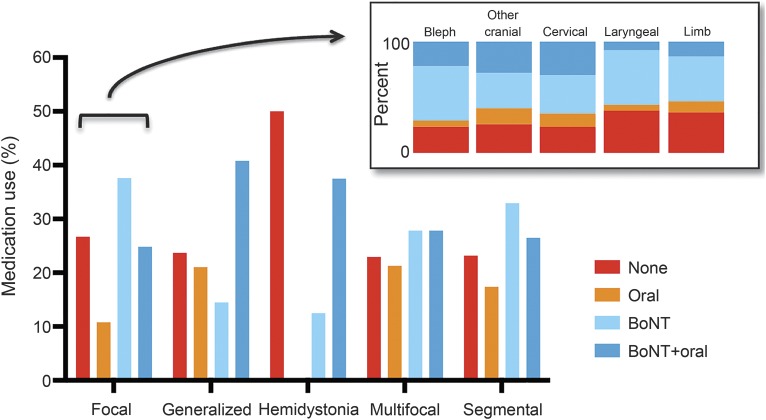
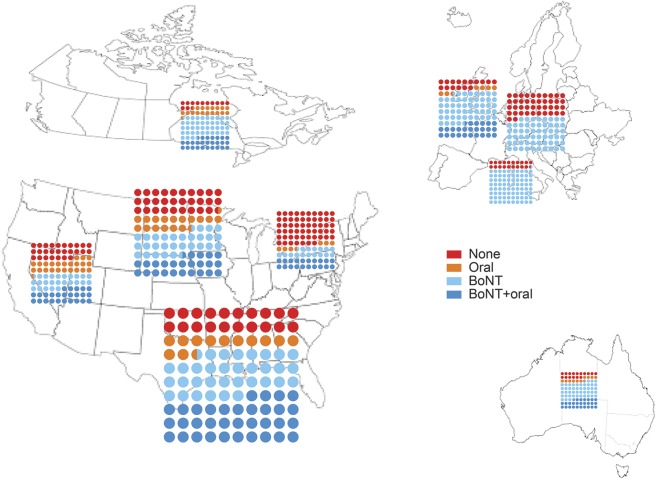
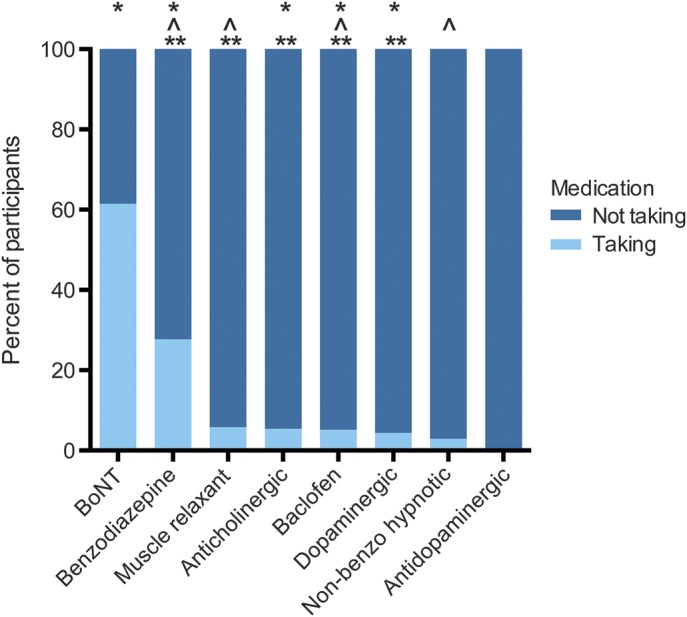
Results: Querying the database for the presence of any medication for dystonia used (includes both injectable and oral therapy), we found 73% using medications (n = 1,488) and 27% using no dystonia medications (n = 538). Furthermore, 61% of the total sample used botulinum toxin (BoNT) therapy alone or in combination. Differences were found in medication use patterns by dystonia type, with the lowest oral medication use in focal dystonia and highest use in generalized dystonia; by region, with highest BoNT therapy rate reported in Italy and the lowest in the Northeast region of the United States; and by focal dystonia subtype, with highest BoNT therapy alone in blepharospasm and spasmodic dysphonia (49%) and lowest in other cranial dystonia (32%).
Conclusions: The majority of patients with dystonia enrolled in the Dystonia Coalition Project 1 were using medications to treat their dystonia. Overall, a complex picture of medication use patterns emerged, with factors such as region, disease duration, type of dystonia, disease severity, and psychiatric comorbidities all playing a significant role.
© 2017 American Academy of Neurology.
Figures
References
-
- Balint B, Bhatia KP. Dystonia: an update on phenomenology, classification, pathogenesis and treatment. Curr Opin Neurol 2014;27:468–476. - PubMed
-
- Comella CL, Leurgans S, Wuu J, Stebbins GT, Chmura T; Dystonia Study Group. Rating scales for dystonia: a multicenter assessment. Mov Disord 2003;18:303–312. - PubMed
-
- Jankovic J. Medical treatment of dystonia. Mov Disord 2013;28:1001–1012. - PubMed
-
- Dressler D, Altenmueller E, Bhidayasiri R, et al. Strategies for treatment of dystonia. J Neural Transm (Vienna) 2016;123:251–258. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical