

Two-Phase Hospital-Associated Outbreak of Mycobacterium abscessus: Investigation and Mitigation
- PMID: 28077517
- PMCID: PMC5848312
- DOI: 10.1093/cid/ciw877
Two-Phase Hospital-Associated Outbreak of Mycobacterium abscessus: Investigation and Mitigation
Abstract
Background: Nontuberculous mycobacteria (NTM) commonly colonize municipal water supplies and cause healthcare-associated outbreaks. We investigated a biphasic outbreak of Mycobacterium abscessus at a tertiary care hospital.
Methods: Case patients had recent hospital exposure and laboratory-confirmed colonization or infection with M. abscessus from January 2013 through December 2015. We conducted a multidisciplinary epidemiologic, field, and laboratory investigation.
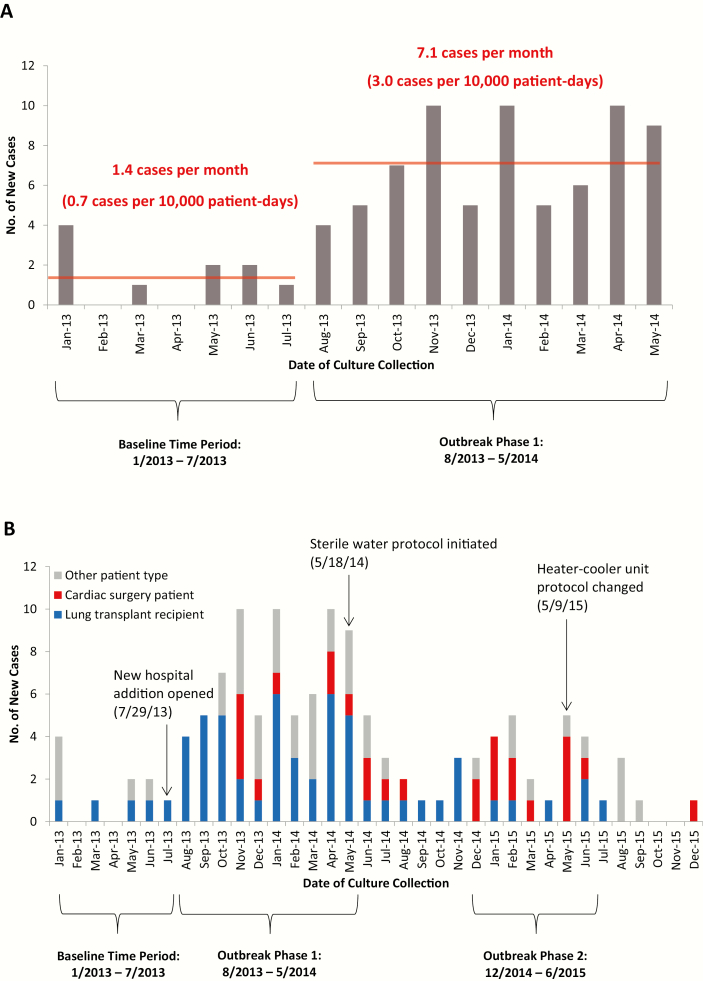
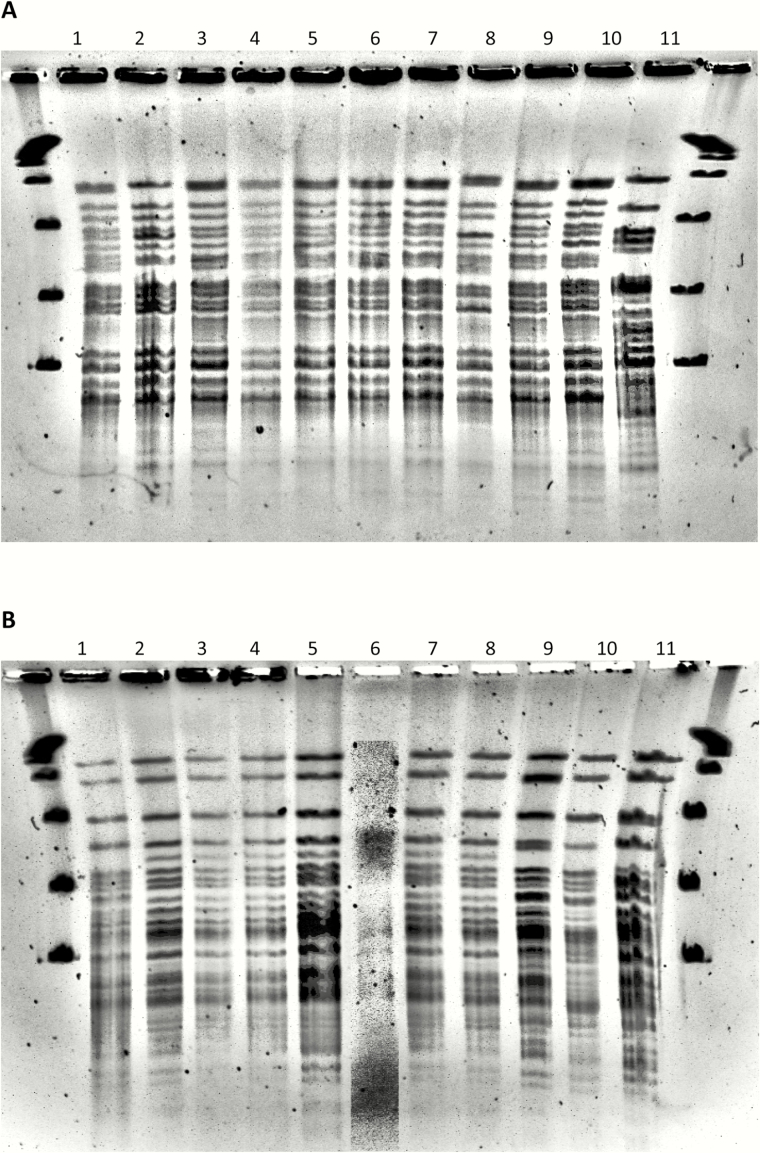
Results: The incidence rate of M. abscessus increased from 0.7 cases per 10000 patient-days during the baseline period (January 2013-July 2013) to 3.0 cases per 10000 patient-days during phase 1 of the outbreak (August 2013-May 2014) (incidence rate ratio, 4.6 [95% confidence interval, 2.3-8.8]; P < .001). Thirty-six of 71 (51%) phase 1 cases were lung transplant patients with positive respiratory cultures. We eliminated tap water exposure to the aerodigestive tract among high-risk patients, and the incidence rate decreased to baseline. Twelve of 24 (50%) phase 2 (December 2014-June 2015) cases occurred in cardiac surgery patients with invasive infections. Phase 2 resolved after we implemented an intensified disinfection protocol and used sterile water for heater-cooler units of cardiopulmonary bypass machines. Molecular fingerprinting of clinical isolates identified 2 clonal strains of M. abscessus; 1 clone was isolated from water sources at a new hospital addition. We made several water engineering interventions to improve water flow and increase disinfectant levels.
Conclusions: We investigated and mitigated a 2-phase clonal outbreak of M. abscessus linked to hospital tap water. Healthcare facilities with endemic NTM should consider similar tap water avoidance and engineering strategies to decrease risk of NTM infection.
Keywords: Mycobacterium abscessus; hospital outbreak; hospital water safety; infection control; nontuberculous mycobacteria.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Modern Healthcare Versus Nontuberculous Mycobacteria: Who Will Have the Upper Hand?Clin Infect Dis. 2017 Apr 1;64(7):912-913. doi: 10.1093/cid/ciw881. Clin Infect Dis. 2017. PMID: 28082270 Free PMC article. No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
