

First-in-Human Evaluation of the Safety and Immunogenicity of an Intranasally Administered Replication-Competent Sendai Virus-Vectored HIV Type 1 Gag Vaccine: Induction of Potent T-Cell or Antibody Responses in Prime-Boost Regimens
- PMID: 28077588
- PMCID: PMC5225252
- DOI: 10.1093/infdis/jiw500
First-in-Human Evaluation of the Safety and Immunogenicity of an Intranasally Administered Replication-Competent Sendai Virus-Vectored HIV Type 1 Gag Vaccine: Induction of Potent T-Cell or Antibody Responses in Prime-Boost Regimens
Abstract
Background: We report the first-in-human safety and immunogenicity assessment of a prototype intranasally administered, replication-competent Sendai virus (SeV)-vectored, human immunodeficiency virus type 1 (HIV-1) vaccine.
Methods: Sixty-five HIV-1-uninfected adults in Kenya, Rwanda, and the United Kingdom were assigned to receive 1 of 4 prime-boost regimens (administered at 0 and 4 months, respectively; ratio of vaccine to placebo recipients, 12:4): priming with a lower-dose SeV-Gag given intranasally, followed by boosting with an adenovirus 35-vectored vaccine encoding HIV-1 Gag, reverse transcriptase, integrase, and Nef (Ad35-GRIN) given intramuscularly (SLA); priming with a higher-dose SeV-Gag given intranasally, followed by boosting with Ad35-GRIN given intramuscularly (SHA); priming with Ad35-GRIN given intramuscularly, followed by boosting with a higher-dose SeV-Gag given intranasally (ASH); and priming and boosting with a higher-dose SeV-Gag given intranasally (SHSH).
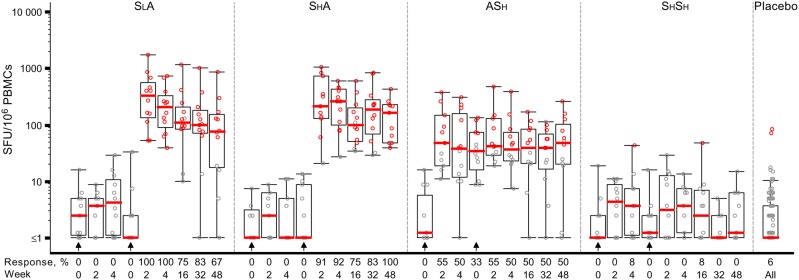
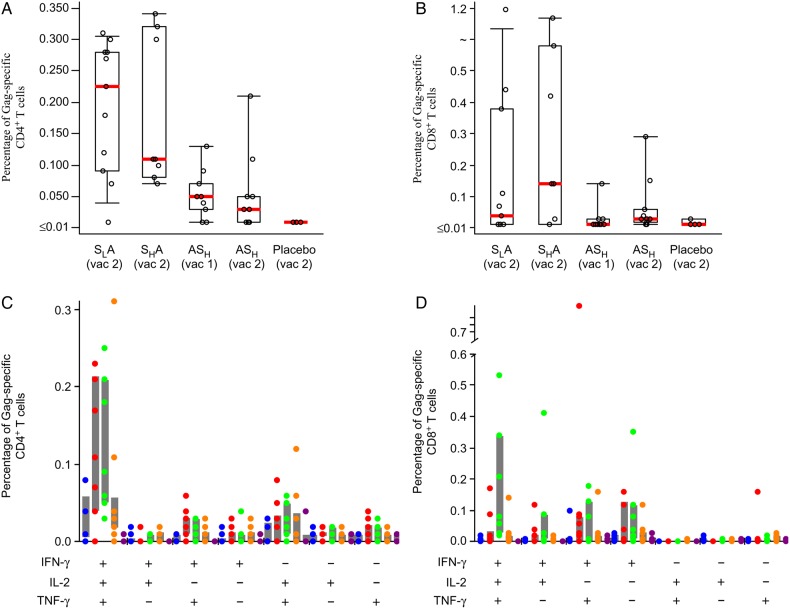
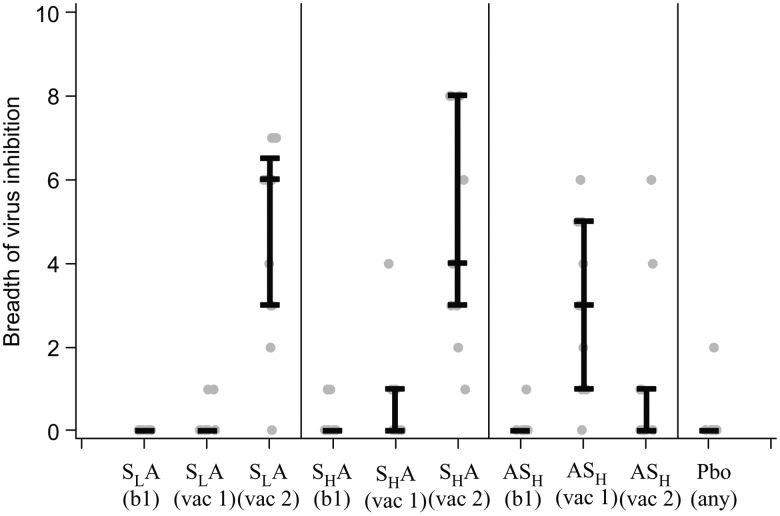
Results: All vaccine regimens were well tolerated. Gag-specific IFN-γ enzyme-linked immunospot-determined response rates and geometric mean responses were higher (96% and 248 spot-forming units, respectively) in groups primed with SeV-Gag and boosted with Ad35-GRIN (SLA and SHA) than those after a single dose of Ad35-GRIN (56% and 54 spot-forming units, respectively) or SeV-Gag (55% and 59 spot-forming units, respectively); responses persisted for ≥8 months after completion of the prime-boost regimen. Functional CD8+ T-cell responses with greater breadth, magnitude, and frequency in a viral inhibition assay were also seen in the SLA and SHA groups after Ad35-GRIN boost, compared with those who received either vaccine alone. SeV-Gag did not boost T-cell counts in the ASH group. In contrast, the highest Gag-specific antibody titers were seen in the ASH group. Mucosal antibody responses were sporadic.
Conclusions: SeV-Gag primed functional, durable HIV-specific T-cell responses and boosted antibody responses. The prime-boost sequence appears to determine which arm of the immune response is stimulated.
Clinical trials registration: NCT01705990.
Keywords: HIV-1 vaccine; Sendai virus vector; adenovirus 35; immunogenicity; intranasal delivery; mucosal responses; prime-boost; replication competent.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures

References
-
- Rerks-Ngarm S, Pitisuttithum P, Nitayaphan S et al. . Vaccination with ALVAC and AIDSVAX to prevent HIV-1 infection in Thailand. N Engl J Med 2009; 361:2209–20. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
