

Hypercalcaemia and hypocalcaemia: finding the balance
- PMID: 28078478
- PMCID: PMC5378747
- DOI: 10.1007/s00520-016-3543-1
Hypercalcaemia and hypocalcaemia: finding the balance
Abstract
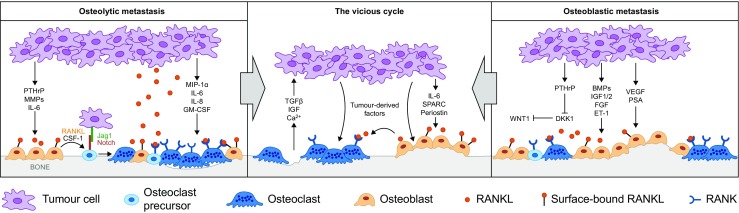
Calcium metabolism in cancer and hypercalcaemia of malignancy: The balance between bone formation and resorption may be disrupted in patients with cancer, leading either to increased bone resorption, calcium release, and possibly hypercalcaemia, or to increased bone formation, sequestration of calcium, and possibly hypocalcaemia. In adults, hypercalcaemia of malignancy is most common in patients with tumours that produce factors that induce osteoclast activation and enhance bone resorption. Impaired renal function and increased renal tubular calcium resorption may further affect calcium levels.
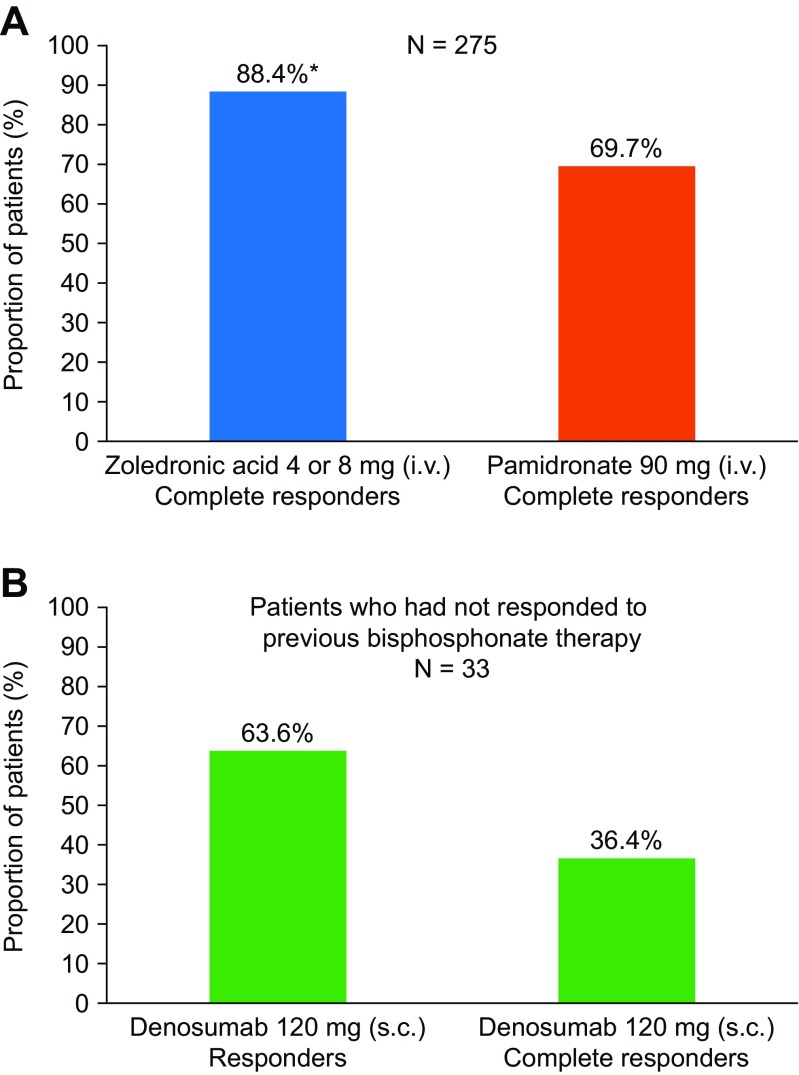
Treatment of hypercalcaemia of malignancy: Inhibitors of bone resorption, first the bisphosphonates and, later, denosumab, have been shown to be effective in hypercalcaemia treatment. Bisphosphonates (which are administered intravenously) are approved for hypercalcaemia of malignancy and are the current mainstay of treatment, whereas denosumab (which is administered subcutaneously) may offer an option for patients who do not respond to bisphosphonates or suffer from renal insufficiency.
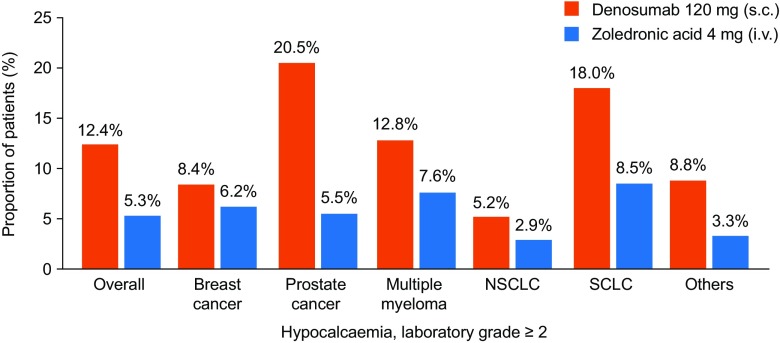
Hypocalcaemia: TREATMENT AND PREVENTION: Hypocalcaemia is most common in patients with prostate cancer and osteoblastic bone metastases, but can occur in patients with a variety of tumour types who are receiving inhibitors of bone resorption. While patients often respond to calcium and vitamin D supplementation, prevention should be the aim; at-risk patients should be identified before starting treatment with inhibitors of bone resorption, be closely monitored during at least the first few months of treatment, and receive concomitant calcium and vitamin D supplementation unless hypercalcaemia is present.
Conclusion: Both hypercalcaemia and hypocalcaemia can be serious if left untreated. It is therefore important that patients with cancer are closely monitored and receive adequate prevention and treatment measures to maintain normal blood calcium levels.
Keywords: Bisphosphonates; Denosumab; Hypercalcaemia; Hypercalcaemia of malignancy; Hypocalcaemia.
Conflict of interest statement
J-JB has served as a consultant for and received lecture fees from Amgen. DN is an employee and shareholder of Amgen. GT has served on advisory board for Celgene, Novartis and Roche.
Figures
Similar articles
-
Hypocalcaemia in patients with prostate cancer treated with a bisphosphonate or denosumab: prevention supports treatment completion.BMC Urol. 2018 Sep 20;18(1):81. doi: 10.1186/s12894-018-0393-9. BMC Urol. 2018. PMID: 30236112 Free PMC article. Review.
-
Managing hypercalcaemia and hypocalcaemia in cancer patients.Curr Opin Support Palliat Care. 2013 Sep;7(3):265-71. doi: 10.1097/SPC.0b013e3283640f5f. Curr Opin Support Palliat Care. 2013. PMID: 23912385 Review.
-
Hypocalcaemia in patients with metastatic bone disease treated with denosumab.Eur J Cancer. 2015 Sep;51(13):1812-21. doi: 10.1016/j.ejca.2015.05.016. Epub 2015 Jun 17. Eur J Cancer. 2015. PMID: 26093811
-
Pitfalls of using denosumab preoperatively to treat refractory severe hypercalcaemia.BMJ Case Rep. 2020 Apr 28;13(4):e233665. doi: 10.1136/bcr-2019-233665. BMJ Case Rep. 2020. PMID: 32350052 Free PMC article.
-
Treatment of hypercalcaemia of malignancy with clodronate.Bone. 1991;12 Suppl 1:S19-23. doi: 10.1016/8756-3282(91)90062-n. Bone. 1991. PMID: 1835397 Review.
Cited by
-
Systematic Review of the Long-Term Effects of Transgender Hormone Therapy on Bone Markers and Bone Mineral Density and Their Potential Effects in Implant Therapy.J Clin Med. 2019 Jun 1;8(6):784. doi: 10.3390/jcm8060784. J Clin Med. 2019. PMID: 31159456 Free PMC article. Review.
-
Hypercalcemia of Malignancy.J Adv Pract Oncol. 2018 Jul-Aug;9(5):496-504. Epub 2018 Jul 1. J Adv Pract Oncol. 2018. PMID: 31086686 Free PMC article. Review.
-
The guiding role of bone metabolism test in osteoporosis treatment.Am J Clin Exp Immunol. 2018 Apr 5;7(2):40-49. eCollection 2018. Am J Clin Exp Immunol. 2018. PMID: 29755856 Free PMC article. Review.
-
Bone Disease in Multiple Myeloma: Biologic and Clinical Implications.Cells. 2022 Jul 27;11(15):2308. doi: 10.3390/cells11152308. Cells. 2022. PMID: 35954151 Free PMC article. Review.
-
Effects of Isoflavone-Rich NADES Extract of Pueraria lobata Roots and Astaxanthin-Rich Phaffia rhodozyma Extract on Prostate Carcinogenesis in Rats.Plants (Basel). 2023 Jan 26;12(3):564. doi: 10.3390/plants12030564. Plants (Basel). 2023. PMID: 36771648 Free PMC article.
References
-
- Ell B, Kang Y (2012) SnapShot: bone metastasis. Cell 151 (3):690–690.e1. doi:10.1016/j.cell.2012.10.005 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
