

Vital Signs: Decrease in Incidence of Diabetes-Related End-Stage Renal Disease among American Indians/Alaska Natives - United States, 1996-2013
- PMID: 28081061
- PMCID: PMC5687264
- DOI: 10.15585/mmwr.mm6601e1
Vital Signs: Decrease in Incidence of Diabetes-Related End-Stage Renal Disease among American Indians/Alaska Natives - United States, 1996-2013
Abstract
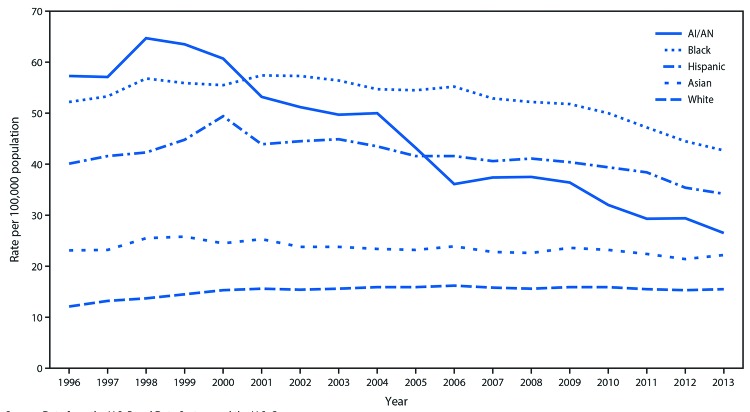
Background: American Indians and Alaska Natives (AI/AN) have the highest diabetes prevalence among any racial/ethnic group in the United States. Among AI/AN, diabetes accounts for 69% of new cases of end-stage renal disease (ESRD), defined as kidney failure treated with dialysis or transplantation. During 1982-1996, diabetes-related ESRD (ESRD-D) in AI/AN increased substantially and disproportionately compared with other racial/ethnic groups.
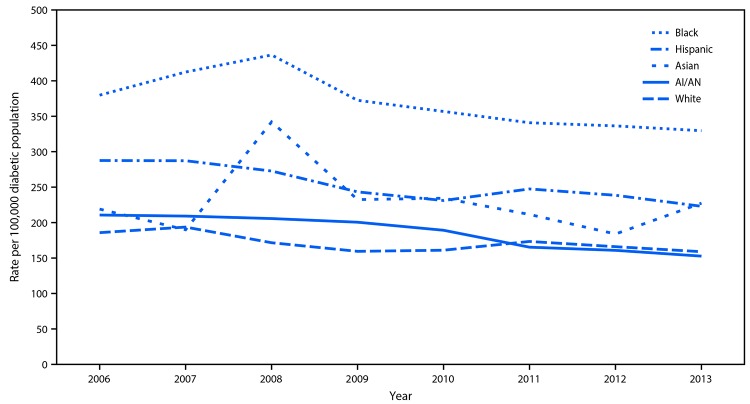
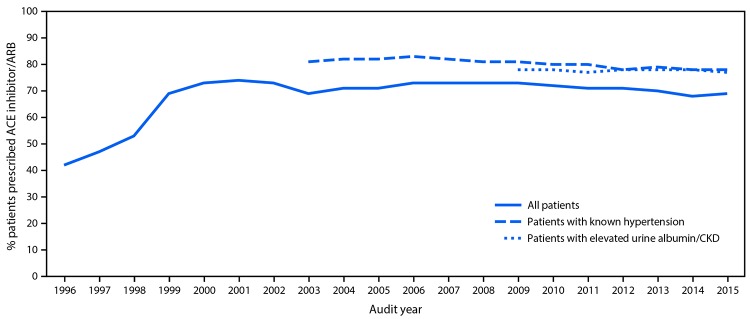
Methods: Data from the U.S. Renal Data System, the Indian Health Service (IHS), the National Health Interview Survey, and the U.S. Census were used to calculate ESRD-D incidence rates by race/ethnicity among U.S. adults aged ≥18 years during 1996-2013 and in the diabetic population during 2006-2013. Rates were age-adjusted based on the 2000 U.S. standard population. IHS clinical data from the Diabetes Cares and Outcomes Audit were analyzed for diabetes management measures in AI/AN.
Results: Among AI/AN adults, age-adjusted ESRD-D rates per 100,000 population decreased 54%, from 57.3 in 1996 to 26.5 in 2013. Although rates for adults in other racial/ethnic groups also decreased during this period, AI/AN had the steepest decline. Among AI/AN with diabetes, ESRD-D incidence decreased during 2006-2013 and, by 2013, was the same as that for whites. Measures related to the assessment and treatment of ESRD-D risk factors also showed more improvement during this period in AI/AN than in the general population.
Conclusion and implications for public health practice: Despite well-documented health and socioeconomic disparities among AI/AN, ESRD-D incidence rates among this population have decreased substantially since 1996. This decline followed implementation by the IHS of public health and population management approaches to diabetes accompanied by improvements in clinical care beginning in the mid-1980s. These approaches might be a useful model for diabetes management in other health care systems, especially those serving populations at high risk.
Figures
Comment in
-
Decreased incidence of end-stage renal disease in American Indians with diabetes: a model for other high-risk populations?Kidney Int. 2017 Apr;91(4):766-768. doi: 10.1016/j.kint.2017.01.027. Kidney Int. 2017. PMID: 28314573
References
-
- United States Renal Data System. USRDS annual data report: Epidemiology of kidney disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, United States Renal. Data Syst 2015;2015. https://www.usrds.org/2015/view/Default.aspx.
-
- CDC. National diabetes statistics report: estimates of diabetes and its burden in the United States, 2014. Atlanta, GA: US Department of Health and Human Services, CDC; 2014. https://www.cdc.gov/diabetes/data/statistics/2014StatisticsReport.html
-
- Zoungas S, de Galan BE, Ninomiya T, et al. ; ADVANCE Collaborative Group. Combined effects of routine blood pressure lowering and intensive glucose control on macrovascular and microvascular outcomes in patients with type 2 diabetes: new results from the ADVANCE trial. Diabetes Care 2009;32:2068–74. 10.2337/dc09-0959 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
