

Management of direct antiviral agent failures
- PMID: 28081594
- PMCID: PMC5266337
- DOI: 10.3350/cmh.2016.0107
Management of direct antiviral agent failures
Abstract
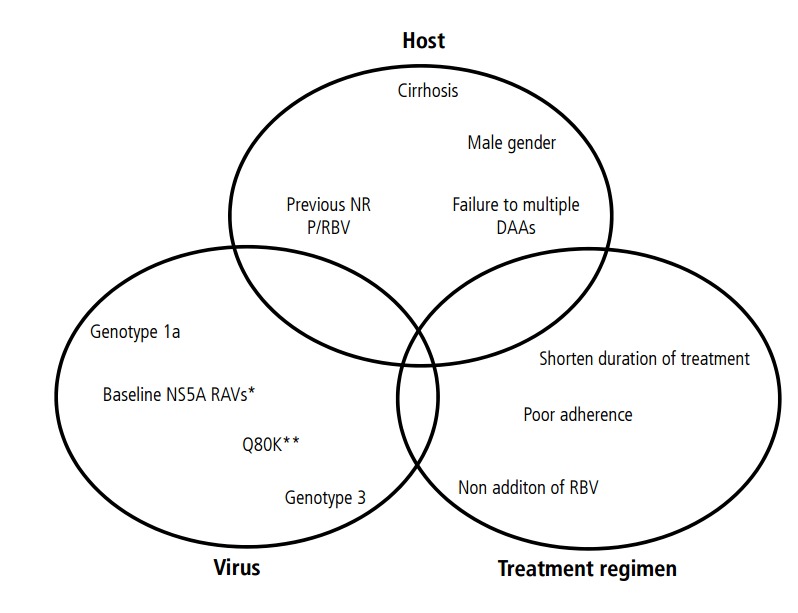
The current standard of care for patients with chronic hepatitis C virus (HCV) infection is a combination of direct-acting antiviral agents (DAAs). Most HCV patients treated with these drugs achieve viral elimination, but 1% to 15% fail to attain this objective. Treatment failures are usually related to relapse, and less often to on-treatment viral breakthrough. HCV drug resistant associated substitutions are detected in most patients who do not eliminate the virus. The risk of developing these variants depends on host- and virus-related factors, the properties of the drugs used, and the treatment strategies applied. Patients who carry Resistant Associated Substitutions (RASs) may not obtain benefits from treatment, and are at a risk of disease progression. Whether HCV RASs persist depends on their type: NS3-4A variants often disappear gradually after DAA therapy is stopped, whereas NS5A variants tend to persist for more than 2 years. The best way to prevent emergence of resistant variants is to eliminate the virus at the first treatment using highly potent DAAs with genetic barriers to resistance. For those who fail an NS5A inhibitor, deferral of treatment is recommended pending the availability of additional data if they do not have cirrhosis or reasons for urgent re-treatment. If re-treatment is needed, the most commonly used strategy is sofosbuvir as backbone therapy plus a drug from a class other than that previously used, for 24 weeks. Unless it is contraindicated, weight-based ribavirin should also be added. If available, nucleotide-based (eg, sofosbuvir) triple or quadruple DAA regimens may be considered. The optimal treatment for patients who fail an NS5A inhibitor and those with multidrug-resistant variants remains to be defined, and research efforts should continue to focus on treatment for these patients.
Keywords: Direct-acting antivirals; Hepatitis C virus; Resistant associated substitutions.
Conflict of interest statement
Maria Buti and Rafael Esteban have received research grants from Gilead and have served as advisors for Gilead, Bristol-Myers Squibb, and Novartis.
Figures
References
-
- Manns MP, von Hahn T. Novel therapies for hepatitis C - one pill fits all? Nat Rev Drug Discov. 2013;12:595–610. - PubMed
-
- Pawlotsky JM. Hepatitis C Virus Resistance to Direct-acting antiviral drugs in interferon-free regimens. Gastroenterology. 2016;151:70–86. - PubMed
-
- American association for the study of the liver (AASLD) and Infectious Diseases Society of America (IDSA) HCV Guidance: Recommendations for testing, managing, and treating hepatitis C. AASLD Web site < www.hcvguidelines.org>, Accessed 17-10-2016. - PubMed
-
- Jensen DM, O’Leary JG, Pockros PJ, Sherman KE, Kwo PY, Mailliard ME, et al. Safety and Efficacy of Sofosbuvir-Containing Regimens for Hepatitis C: Real-World Experience in a Diverse, Longitudinal Observational Cohort. Hepatology. 2014;60(Suppl 1):S219.
-
- Bacon BR, Dieterich D, Flamm SL, Kowdley KV, Lawitz E, Milligan S, et al. Efficacy of sofosbuvir and simeprevir-based regimens for 304 HCV treatment-experienced patients in a reallife setting; data from the TRIO network. Hepatology. 2014;60(Suppl 1):S672.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
