

The Role of Extent of Surgical Resection and Lymph Node Assessment for Clinical Stage I Pulmonary Lepidic Adenocarcinoma: An Analysis of 1991 Patients
- PMID: 28082103
- PMCID: PMC5367982
- DOI: 10.1016/j.jtho.2017.01.003
The Role of Extent of Surgical Resection and Lymph Node Assessment for Clinical Stage I Pulmonary Lepidic Adenocarcinoma: An Analysis of 1991 Patients
Abstract
Background: This study examined the association of extent of lung resection, pathologic nodal evaluation, and survival for patients with clinical stage I (cT1-2N0M0) adenocarcinoma with lepidic histologic features in the National Cancer Data Base.
Methods: The association between extent of surgical resection and long-term survival for patients in the National Cancer Data Base with clinical stage I lepidic adenocarcinoma who underwent lobectomy or sublobar resection was evaluated using Kaplan-Meier and Cox proportional hazards regression analyses.
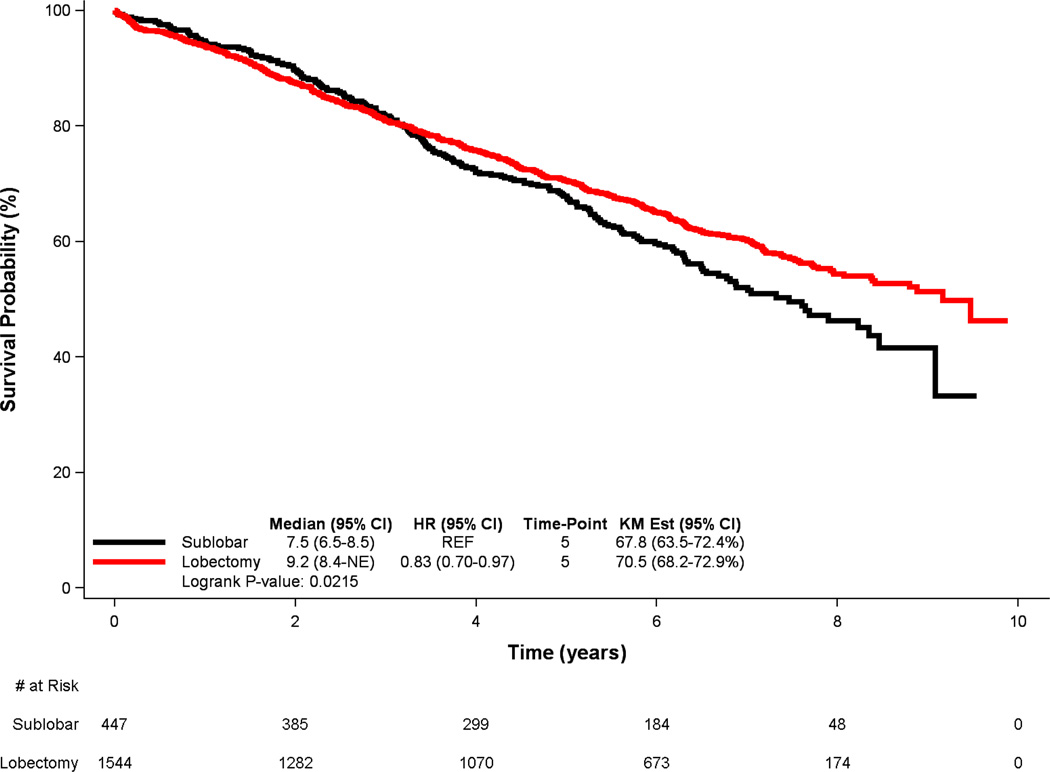
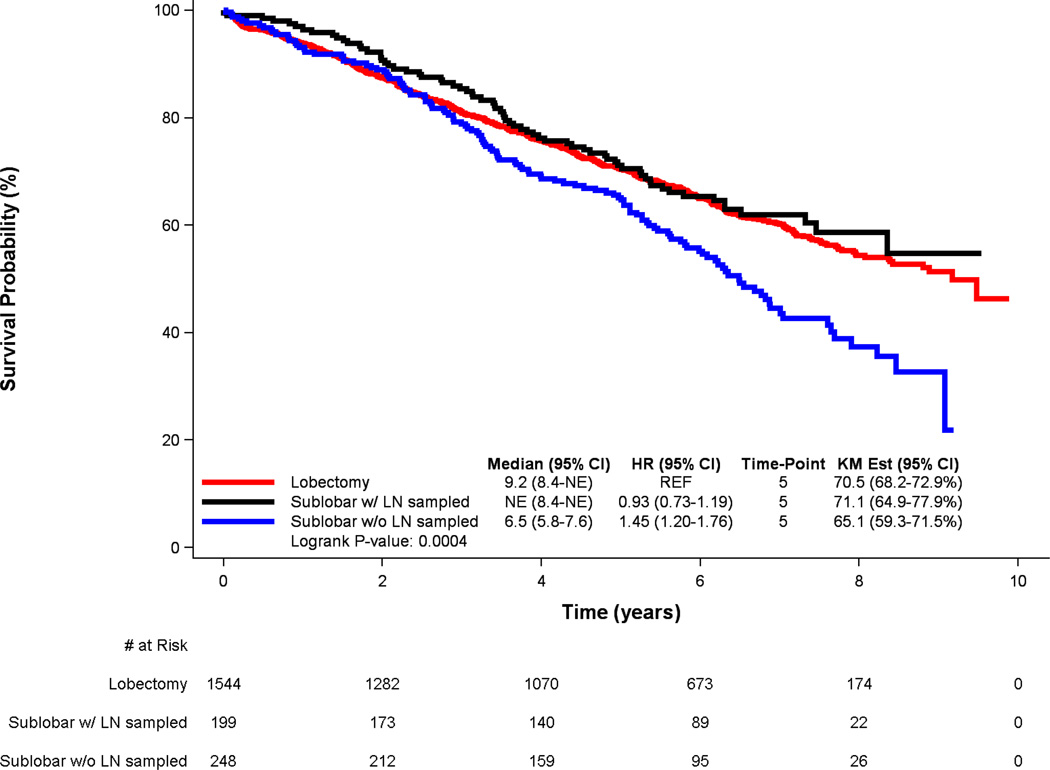
Results: Of the 1991 patients with cT1-2N0M0 lepidic adenocarcinoma who met the study criteria, 1544 underwent lobectomy and 447 underwent sublobar resection. Patients treated with sublobar resection were older, more likely to be female, and had higher Charlson/Deyo comorbidity scores, but they had smaller tumors and lower T status. Of the patients treated with lobectomy, 6% (n = 92) were upstaged because of positive nodal disease, with a median of seven lymph nodes sampled (interquartile range 4-10). In an analysis of the entire cohort, lobectomy was associated with a significant survival advantage over sublobar resection in univariate analysis (median survival 9.2 versus 7.5 years, p = 0.022, 5-year survival 70.5% versus 67.8%) and after multivariable adjustment (hazard ratio = 0.81, 95% confidence interval: 0.68-0.95, p = 0.011). However, lobectomy was no longer independently associated with improved survival when compared with sublobar resection (hazard ratio = 0.99, 95% confidence interval: 0.77-1.27, p = 0.905) in a multivariable analysis of a subset of patients in which only those patients who had undergone a sublobar resection including lymph node sampling were compared with patients treated with lobectomy.
Conclusions: Surgeons treating patients with stage I lung adenocarcinoma with lepidic features should cautiously utilize sublobar resection rather than lobectomy, and they must always perform adequate pathologic lymph node evaluation.
Keywords: Bronchioloalveolar carcinoma; Lepidic adenocarcinoma; Lymph node dissection; Non–small cell lung cancer; Thoracic surgery.
Copyright © 2017 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Breathnach OS, Kwiatkowski DJ, Finkelstein DM, Godleski J, Sugarbaker DJ, Johnson BE, et al. Bronchioloalveolar carcinoma of the lung: recurrences and survival in patients with stage I disease. J Thorac Cardiovasc Surg. 2001;121(1):42–47. - PubMed
-
- Nakagiri T, Sawabata N, Morii E, Inoue M, Shintani Y, Funaki S, et al. Evaluation of the new IASLC/ATS/ERS proposed classification of adenocarcinoma based on lepidic pattern in patients with pathological stage IA pulmonary adenocarcinoma. Gen Thorac Cardiovasc Surg. 2014;62(11):671–677. - PubMed
-
- Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International Association for the study of lung cancer/American Thoracic Society/European Respiratory Society: international multidisciplinary classification of lung adenocarcinoma: executive summary. Proc Am Thorac Soc. 2011;8(5):381–385. - PubMed
-
- Read WL, Page NC, Tierney RM, Piccirillo JF, Govindan R. The epidemiology of bronchioloalveolar carcinoma over the past two decades: analysis of the SEER database. Lung Cancer. 2004;45(2):137–142. - PubMed
-
- Barsky SH, Cameron R, Osann KE, Tomita D, Holmes EC. Rising incidence of bronchioloalveolar lung carcinoma and its unique clinicopathologic features. Cancer. 1994;73(4):1163–1170. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
