

Defining the genetic architecture of hypertrophic cardiomyopathy: re-evaluating the role of non-sarcomeric genes
- PMID: 28082330
- PMCID: PMC5837460
- DOI: 10.1093/eurheartj/ehw603
Defining the genetic architecture of hypertrophic cardiomyopathy: re-evaluating the role of non-sarcomeric genes
Abstract
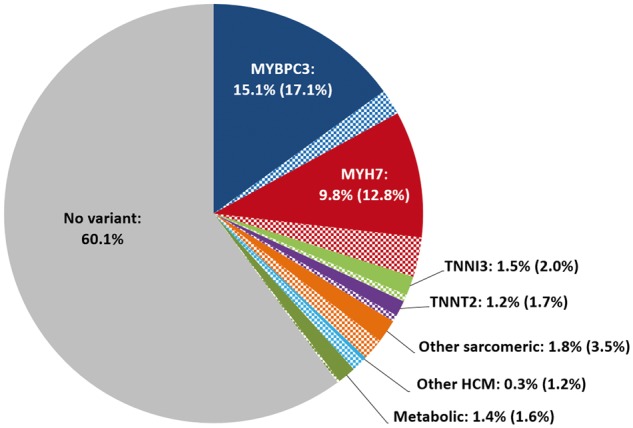
Aim: Hypertrophic cardiomyopathy (HCM) exhibits genetic heterogeneity that is dominated by variation in eight sarcomeric genes. Genetic variation in a large number of non-sarcomeric genes has also been implicated in HCM but not formally assessed. Here we used very large case and control cohorts to determine the extent to which variation in non-sarcomeric genes contributes to HCM.
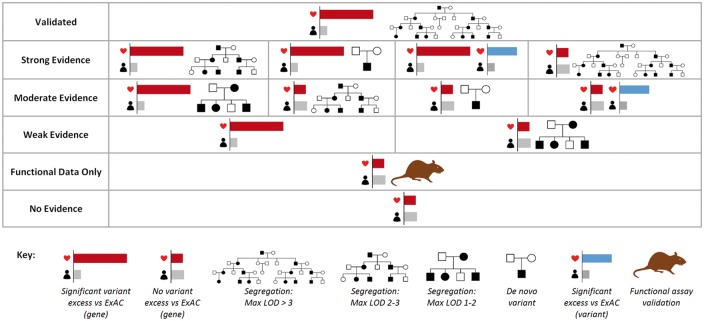
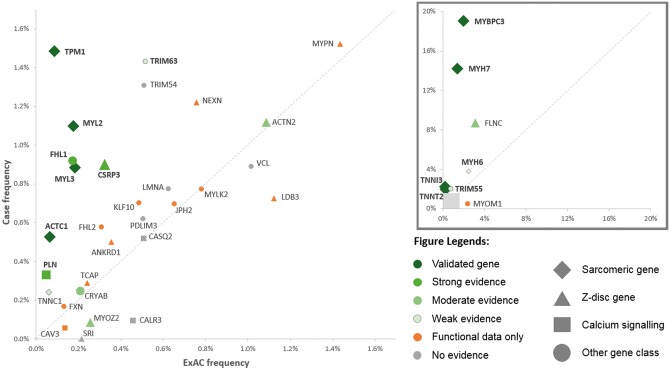
Methods and results: We sequenced known and putative HCM genes in a new large prospective HCM cohort (n = 804) and analysed data alongside the largest published series of clinically genotyped HCM patients (n = 6179), previously published HCM cohorts and reference population samples from the exome aggregation consortium (ExAC, n = 60 706) to assess variation in 31 genes implicated in HCM. We found no significant excess of rare (minor allele frequency < 1:10 000 in ExAC) protein-altering variants over controls for most genes tested and conclude that novel variants in these genes are rarely interpretable, even for genes with previous evidence of co-segregation (e.g. ACTN2). To provide an aid for variant interpretation, we integrated HCM gene sequence data with aggregated pedigree and functional data and suggest a means of assessing gene pathogenicity in HCM using this evidence.
Conclusion: We show that genetic variation in the majority of non-sarcomeric genes implicated in HCM is not associated with the condition, reinforce the fact that the sarcomeric gene variation is the primary cause of HCM known to date and underscore that the aetiology of HCM is unknown in the majority of patients.
Keywords: ExAC; HCM genetics; Hypertrophic cardiomyopathy; Mendelian genetics; Rare genetic variation.
© The Author 2017. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Other side of the coin: the missing heritability in hypertrophic cardiomyopathy.Eur Heart J. 2017 Dec 7;38(46):3469-3471. doi: 10.1093/eurheartj/ehx024. Eur Heart J. 2017. PMID: 28201496 No abstract available.
References
-
- Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE.. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary artery risk development in (Young) adults. Circulation 1995;92:785–789. - PubMed
-
- Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA 2002;287:1308–1320. - PubMed
-
- Jarcho JA, McKenna W, Pare JA, Solomon SD, Holcombe RF, Dickie S, Levi T, Donis-Keller H, Seidman JG, Seidman CE.. Mapping a gene for familial hypertrophic cardiomyopathy to chromosome 14q1. N Engl J Med 1989;321:1372–1378. - PubMed
-
- Maron BJ, Maron MS, Semsarian C.. Genetics of hypertrophic cardiomyopathy after 20 years: clinical perspectives. J Am Coll Cardiol 2012;60:705–715. - PubMed
-
- Lek M, Karczewski KJ, Minikel EV, Samocha KE, Banks E, Fennell T, O’donnell-Luria AH, Ware JS, Hill AJ, Cummings BB, Tukiainen T, Birnbaum DP, Kosmicki JA, Duncan LE, Estrada K, Zhao F, Zou J, Pierce-Hoffman E, Berghout J, Cooper DN, Deflaux N, DePristo M, Do R, Flannick J, Fromer M, Gauthier L, Goldstein J, Gupta N, Howrigan D, Kiezun A, Kurki MI, Moonshine AL, Natarajan P, Orozco L, Peloso GM, Poplin R, Rivas MA, Ruano-Rubio V, Rose SA, Ruderfer DM, Shakir K, Stenson PD, Stevens C, Thomas BP, Tiao G, Tusie-Luna MT, Weisburd B, Won HH, Yu D, Altshuler DM, Ardissino D, Boehnke M, Danesh J, Donnelly S, Elosua R, Florez JC, Gabriel SB, Getz G, Glatt SJ, Hultman CM, Kathiresan S, Laakso M, McCarroll S, McCarthy MI, McGovern D, McPherson R, Neale BM, Palotie A, Purcell SM, Saleheen D, Scharf JM, Sklar P, Sullivan PF, Tuomilehto J, Tsuang MT, Watkins HC, Wilson JG, Daly MJ, MacArthur DG; Exome Aggregation Consortium. Analysis of protein-coding genetic variation in 60,706 humans. Nature 2016;536:285–291. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
