

High-Intensity Interval Training in Patients With Heart Failure With Reduced Ejection Fraction
- PMID: 28082387
- PMCID: PMC5325251
- DOI: 10.1161/CIRCULATIONAHA.116.022924
High-Intensity Interval Training in Patients With Heart Failure With Reduced Ejection Fraction
Abstract
Background: Small studies have suggested that high-intensity interval training (HIIT) is superior to moderate continuous training (MCT) in reversing cardiac remodeling and increasing aerobic capacity in patients with heart failure with reduced ejection fraction. The present multicenter trial compared 12 weeks of supervised interventions of HIIT, MCT, or a recommendation of regular exercise (RRE).
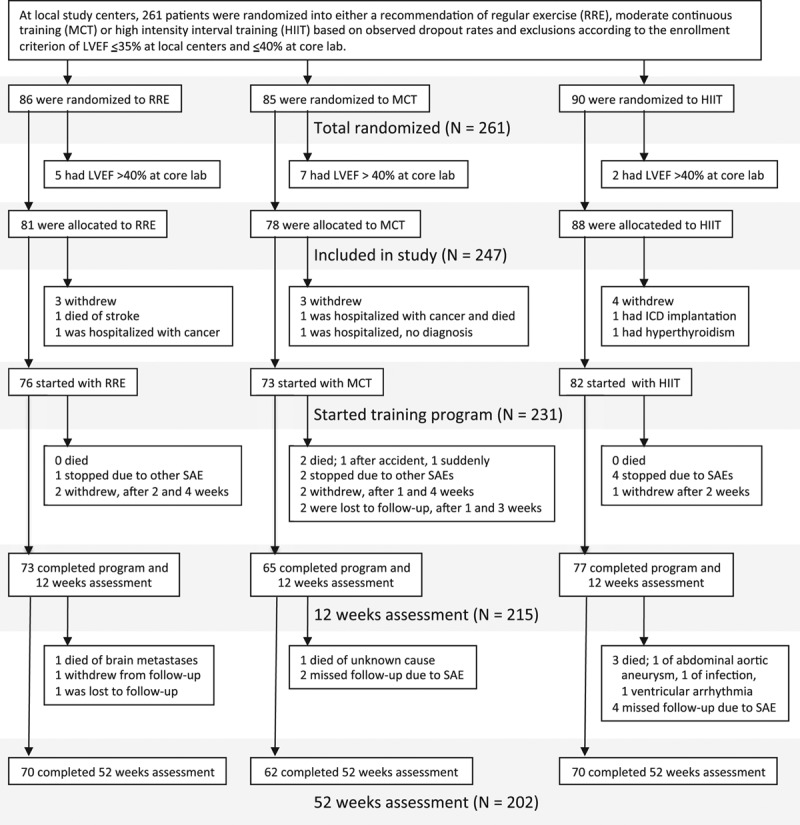
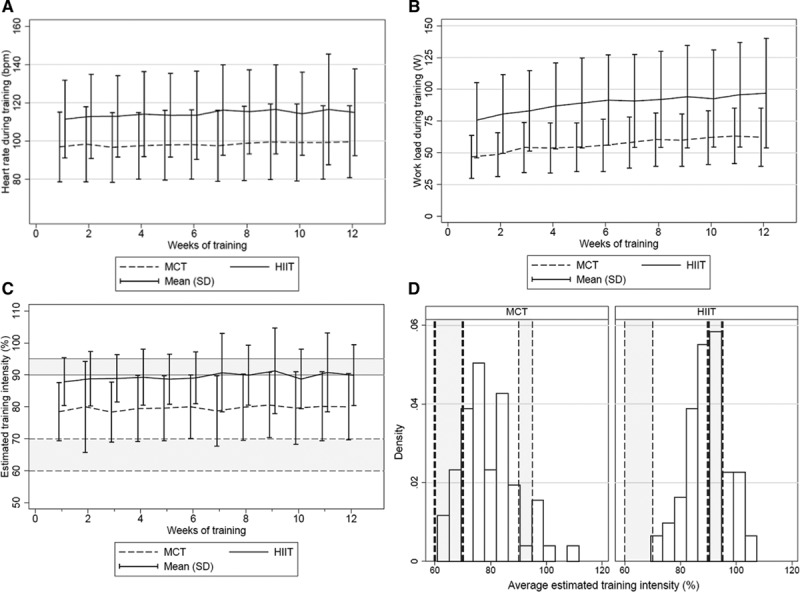
Methods: Two hundred sixty-one patients with left ventricular ejection fraction ≤35% and New York Heart Association class II to III were randomly assigned to HIIT at 90% to 95% of maximal heart rate, MCT at 60% to 70% of maximal heart rate, or RRE. Thereafter, patients were encouraged to continue exercising on their own. Clinical assessments were performed at baseline, after the intervention, and at follow-up after 52 weeks. Primary end point was a between-group comparison of change in left ventricular end-diastolic diameter from baseline to 12 weeks.
Results: Groups did not differ in age (median, 60 years), sex (19% women), ischemic pathogenesis (59%), or medication. Change in left ventricular end-diastolic diameter from baseline to 12 weeks was not different between HIIT and MCT (P=0.45); left ventricular end-diastolic diameter changes compared with RRE were -2.8 mm (-5.2 to -0.4 mm; P=0.02) in HIIT and -1.2 mm (-3.6 to 1.2 mm; P=0.34) in MCT. There was also no difference between HIIT and MCT in peak oxygen uptake (P=0.70), but both were superior to RRE. However, none of these changes was maintained at follow-up after 52 weeks. Serious adverse events were not statistically different during supervised intervention or at follow-up at 52 weeks (HIIT, 39%; MCT, 25%; RRE, 34%; P=0.16). Training records showed that 51% of patients exercised below prescribed target during supervised HIIT and 80% above target in MCT.
Conclusions: HIIT was not superior to MCT in changing left ventricular remodeling or aerobic capacity, and its feasibility remains unresolved in patients with heart failure.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00917046.
Keywords: exercise; heart failure.
© 2017 The Authors.
Figures
Comment in
-
Letter by Iellamo and Volterrani Regarding Article, "High-Intensity Interval Training in Patients With Heart Failure With Reduced Ejection Fraction".Circulation. 2017 Aug 8;136(6):605-606. doi: 10.1161/CIRCULATIONAHA.117.028249. Circulation. 2017. PMID: 28784830 No abstract available.
-
Letter by Wisløff et al Regarding Article, "High-Intensity Interval Training in Patients With Heart Failure With Reduced Ejection Fraction".Circulation. 2017 Aug 8;136(6):607-608. doi: 10.1161/CIRCULATIONAHA.117.028318. Circulation. 2017. PMID: 28784831 No abstract available.
-
Letter by Bianchi Regarding Article, "High-Intensity Interval Training in Patients With Heart Failure With Reduced Ejection Fraction".Circulation. 2017 Aug 8;136(6):609-610. doi: 10.1161/CIRCULATIONAHA.117.028668. Circulation. 2017. PMID: 28784832 No abstract available.
-
Response by Ellingsen et al to Letters Regarding Article, "High-Intensity Interval Training in Patients With Heart Failure With Reduced Ejection Fraction".Circulation. 2017 Aug 8;136(6):611-612. doi: 10.1161/CIRCULATIONAHA.117.029145. Circulation. 2017. PMID: 28784833 No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P Authors/Task Force Members. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128. - PubMed
-
- Vanhees L, Rauch B, Piepoli M, van Buuren F, Takken T, Börjesson M, Bjarnason-Wehrens B, Doherty P, Dugmore D, Halle M Writing Group, EACPR. Importance of characteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular disease (part III). Eur J Prev Cardiol. 2012;19:1333–1356. doi: 10.1177/2047487312437063. - PubMed
-
- O’Connor CM, Whellan DJ, Lee KL, Keteyian SJ, Cooper LS, Ellis SJ, Leifer ES, Kraus WE, Kitzman DW, Blumenthal JA, Rendall DS, Miller NH, Fleg JL, Schulman KA, McKelvie RS, Zannad F, Piña IL HF-ACTION Investigators. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA. 2009;301:1439–1450. doi: 10.1001/jama.2009.454. - PMC - PubMed
-
- Wisløff U, Støylen A, Loennechen JP, Bruvold M, Rognmo Ø, Haram PM, Tjønna AE, Helgerud J, Slørdahl SA, Lee SJ, Videm V, Bye A, Smith GL, Najjar SM, Ellingsen Ø, Skjaerpe T. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: a randomized study. Circulation. 2007;115:3086–3094. doi: 10.1161/CIRCULATIONAHA.106.675041. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
