

Vancomycin-Associated Cast Nephropathy
- PMID: 28082518
- PMCID: PMC5461798
- DOI: 10.1681/ASN.2016080867
Vancomycin-Associated Cast Nephropathy
Abstract
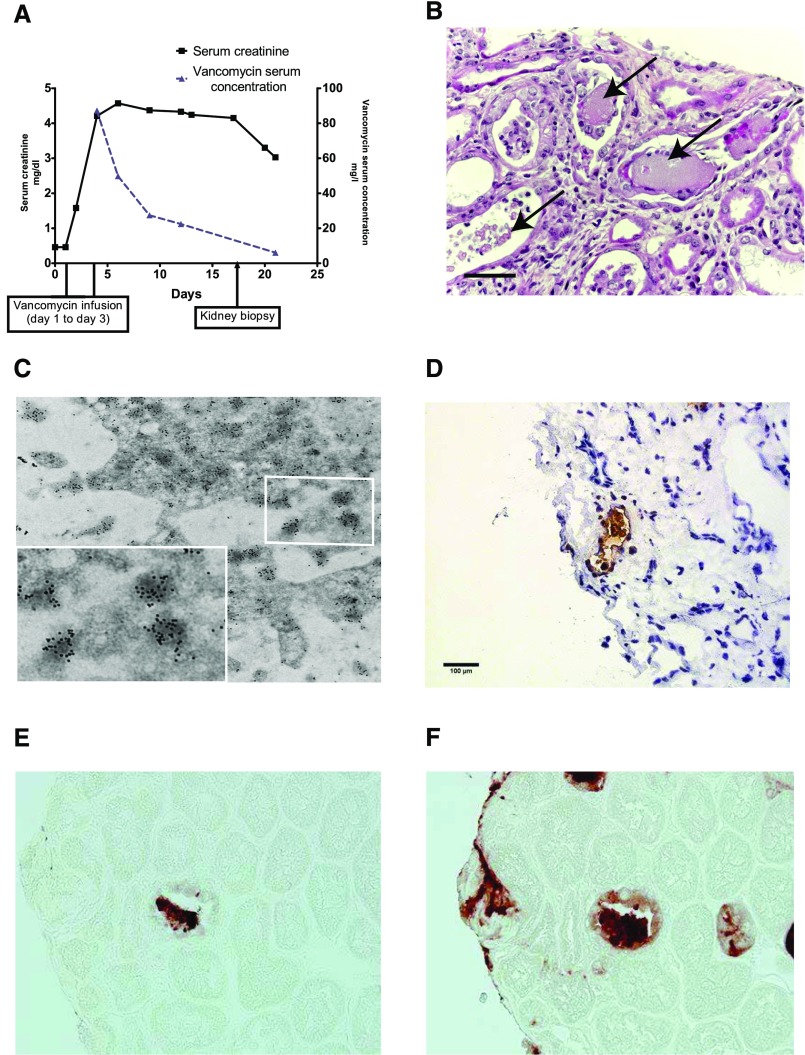
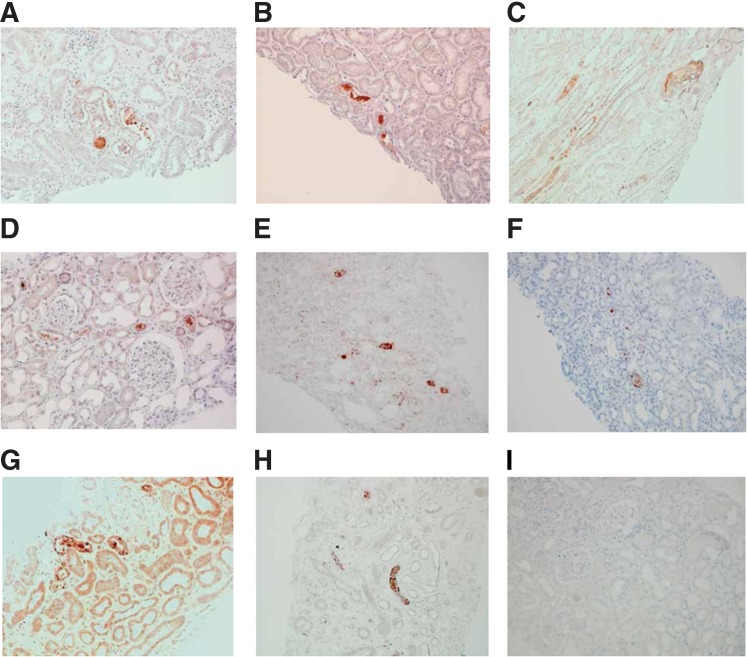
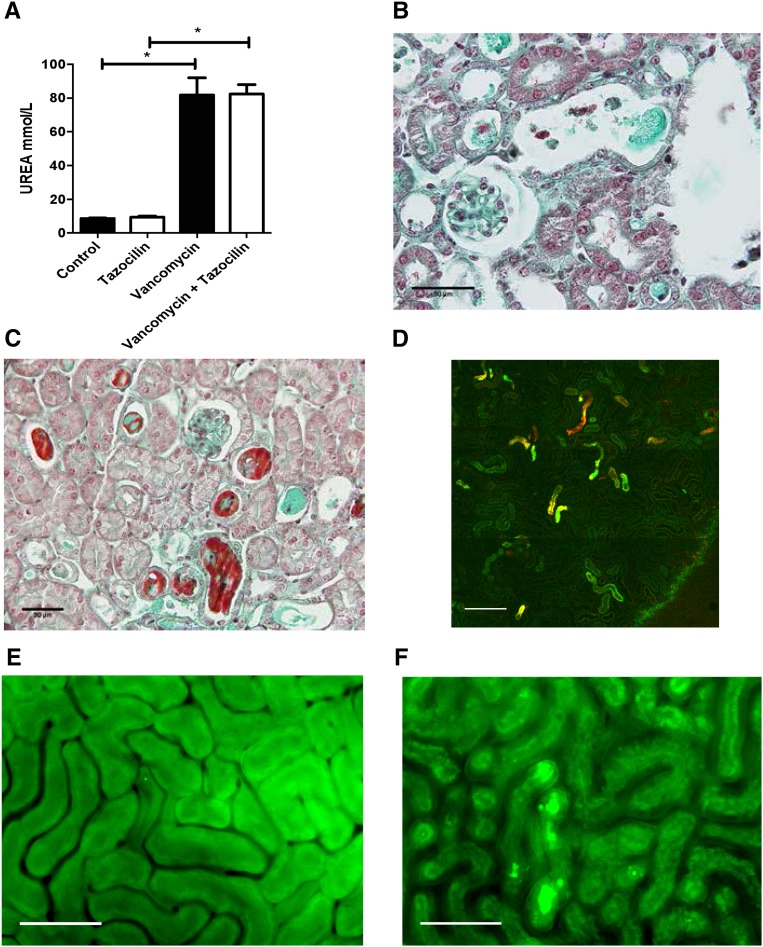
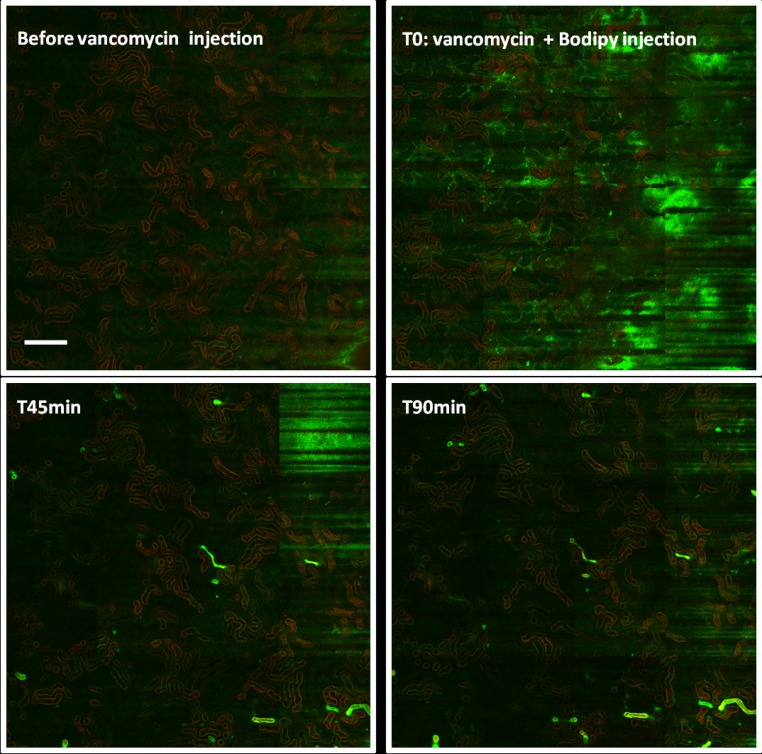
Vancomycin is a widely prescribed antibiotic, but the exact nature of vancomycin-associated nephrotoxicity is unclear, in particular when considering the frequent coadministration of aminoglycosides. We describe here the initial case of a 56-year-old woman with normal renal function developing unexplained ARF without hypovolemia after administration of vancomycin without coadministration of aminoglycosides. Studying the patient's renal biopsy specimen, we ascertained that obstructive tubular casts composed of noncrystal nanospheric vancomycin aggregates entangled with uromodulin explained the vancomycin-associated ARF. We developed in parallel a new immunohistologic staining technique to detect vancomycin in renal tissue and confirmed retrospectively that deleterious vancomycin-associated casts existed in eight additional patients with acute tubular necrosis in the absence of hypovolemia. Concomitant high vancomycin trough plasma levels had been observed in each patient. We also reproduced experimentally the toxic and obstructive nature of vancomycin-associated cast nephropathy in mice, which we detected using different in vivo imaging techniques. In conclusion, the interaction of uromodulin with nanospheric vancomycin aggregates represents a new mode of tubular cast formation, revealing the hitherto unsuspected mechanism of vancomycin-associated renal injury.
Keywords: acute renal failure; acute tubular necrosis; tubular cast; tubular epithelium; vancomycin.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Vancomycin in the Kidney-A Novel Cast Nephropathy.J Am Soc Nephrol. 2017 Jun;28(6):1669-1670. doi: 10.1681/ASN.2017010091. Epub 2017 Mar 7. J Am Soc Nephrol. 2017. PMID: 28270410 Free PMC article. No abstract available.
References
-
- Griffith RS: Introduction to vancomycin. Rev Infect Dis 3[Suppl]: S200–S204, 1981 - PubMed
-
- Levine DP: Vancomycin: A history. Clin Infect Dis 42[Suppl 1]: S5–S12, 2006 - PubMed
-
- Oktem F, Arslan MK, Ozguner F, Candir O, Yilmaz HR, Ciris M, Uz E: In vivo evidences Suggesting the role of oxidative stress in pathogenesis of vancomycin-induced nephrotoxicity: Protection by erdosteine. Toxicology 215: 227–233, 2005 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
