

Right Ventricular Structure and Function Are Associated With Incident Atrial Fibrillation: MESA-RV Study (Multi-Ethnic Study of Atherosclerosis-Right Ventricle)
- PMID: 28082528
- PMCID: PMC5261825
- DOI: 10.1161/CIRCEP.116.004738
Right Ventricular Structure and Function Are Associated With Incident Atrial Fibrillation: MESA-RV Study (Multi-Ethnic Study of Atherosclerosis-Right Ventricle)
Abstract
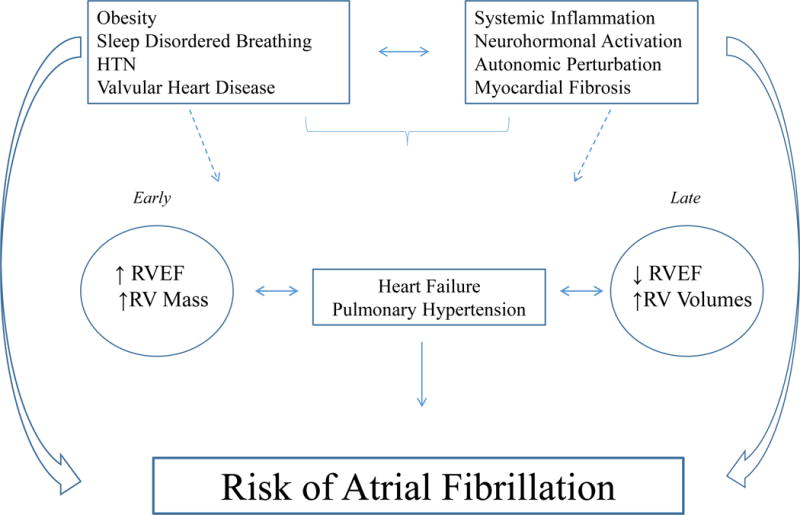
Background: Right ventricular (RV) morphology has been associated with drivers of atrial fibrillation (AF) risk, including left ventricular and pulmonary pathology, systemic inflammation, and neurohormonal activation. The aim of this study was to investigate the association between RV morphology and risk of incident AF.
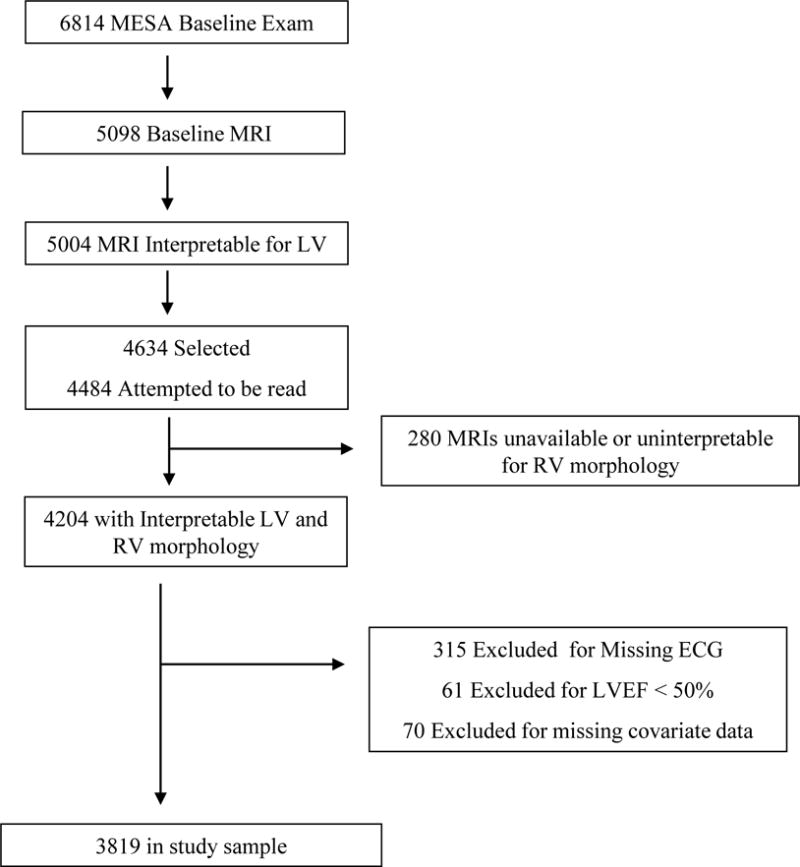
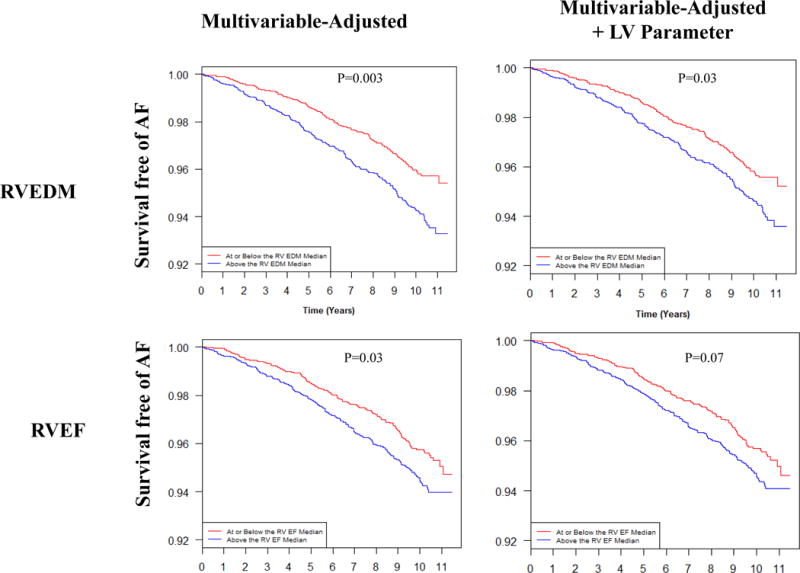
Methods and results: We interpreted cardiac magnetic resonance imaging in 4204 participants free of clinical cardiovascular disease in the MESA (Multi-Ethnic Study of Atherosclerosis). Incident AF was determined using hospital discharge records, study electrocardiograms, and Medicare claims data. The study sample (n=3819) was 61±10 years old and 47% male with 47.2% current/former smokers. After adjustment for demographics and clinical factors, including incident heart failure, higher RV ejection fraction (hazard ratio, 1.16 per SD; 95% confidence interval, 1.03-1.32; P=0.02) and greater RV mass (hazard ratio, 1.25 per SD; 95% confidence interval, 1.08-1.44; P=0.002) were significantly associated with incident AF. After additional adjustment for the respective left ventricular parameter, higher RV ejection fraction remained significantly associated with incident AF (hazard ratio, 1.15 per SD; 95% confidence interval, 1.01-1.32; P=0.04), whereas the association was attenuated for RV mass (hazard ratio, 1.16 per SD; 95% confidence interval, 0.99-1.35; P=0.07). In a subset of patients with available spirometry (n=2540), higher RV ejection fraction and mass remained significantly associated with incident AF after additional adjustment for lung function (P=0.02 for both).
Conclusions: Higher RV ejection fraction and greater RV mass were associated with an increased risk of AF in a multiethnic population free of clinical cardiovascular disease at baseline.
Keywords: atrial fibrillation; heart failure; heart ventricles; magnetic resonance imaging.
© 2017 American Heart Association, Inc.
Figures
References
-
- Menke J, Luthje L, Kastrup A, Larsen J. Thromboembolism in atrial fibrillation. Am J Cardiol. 2010;105:502–510. - PubMed
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. - PubMed
-
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton-Cheh C, Lubitz SA, Magnani JW, Ellinor PT, Seshadri S, Wolf PA, Vasan RS, Benjamin EJ, Levy D. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154–162. - PMC - PubMed
-
- Van Wagoner DR, Piccini JP, Albert CM, Anderson ME, Benjamin EJ, Brundel B, Califf RM, Calkins H, Chen PS, Chiamvimonvat N, Darbar D, Eckhardt LL, Ellinor PT, Exner DV, Fogel RI, Gillis AM, Healey J, Hohnloser SH, Kamel H, Lathrop DA, Lip GY, Mehra R, Narayan SM, Olgin J, Packer D, Peters NS, Roden DM, Ross HM, Sheldon R, Wehrens XH. Progress toward the prevention and treatment of atrial fibrillation: A summary of the Heart Rhythm Society Research Forum on the Treatment and Prevention of Atrial Fibrillation, Washington, DC, December 9–10, 2013. Heart Rhythm. 2015;12:e5–e29. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
