

Liver fibrosis and hepatic stellate cells: Etiology, pathological hallmarks and therapeutic targets
- PMID: 28082803
- PMCID: PMC5192262
- DOI: 10.3748/wjg.v22.i48.10512
Liver fibrosis and hepatic stellate cells: Etiology, pathological hallmarks and therapeutic targets
Abstract
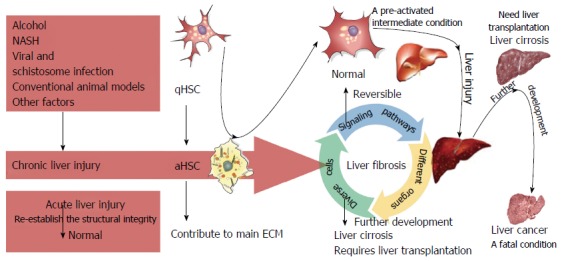
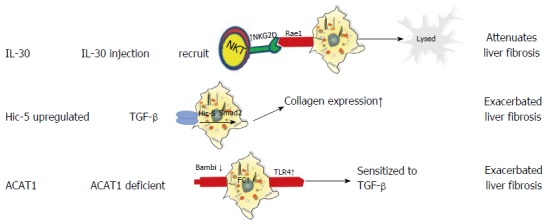
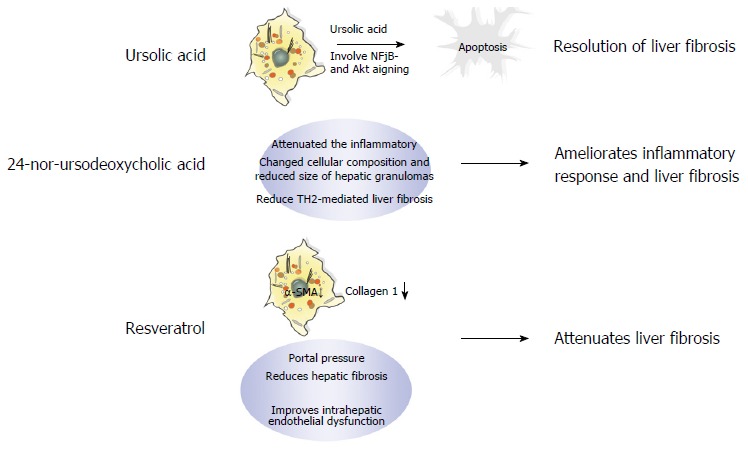
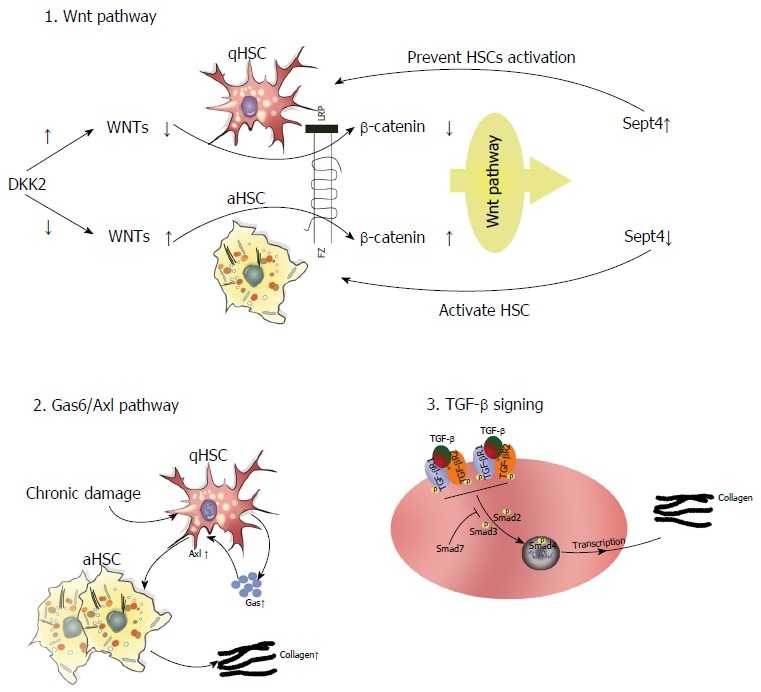
Liver fibrosis is a reversible wound-healing process aimed at maintaining organ integrity, and presents as the critical pre-stage of liver cirrhosis, which will eventually progress to hepatocellular carcinoma in the absence of liver transplantation. Fibrosis generally results from chronic hepatic injury caused by various factors, mainly viral infection, schistosomiasis, and alcoholism; however, the exact pathological mechanisms are still unknown. Although numerous drugs have been shown to have antifibrotic activity in vitro and in animal models, none of these drugs have been shown to be efficacious in the clinic. Importantly, hepatic stellate cells (HSCs) play a key role in the initiation, progression, and regression of liver fibrosis by secreting fibrogenic factors that encourage portal fibrocytes, fibroblasts, and bone marrow-derived myofibroblasts to produce collagen and thereby propagate fibrosis. These cells are subject to intricate cross-talk with adjacent cells, resulting in scarring and subsequent liver damage. Thus, an understanding of the molecular mechanisms of liver fibrosis and their relationships with HSCs is essential for the discovery of new therapeutic targets. This comprehensive review outlines the role of HSCs in liver fibrosis and details novel strategies to suppress HSC activity, thereby providing new insights into potential treatments for liver fibrosis.
Keywords: Etiology; Fibrosis; Hepatic stellate cells; Liver cirrhosis; Pathology; Treatment.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
References
-
- Weiskirchen R, Tacke F. Liver Fibrosis: From Pathogenesis to Novel Therapies. Dig Dis. 2016;34:410–422. - PubMed
-
- Pinzani M. Pathophysiology of Liver Fibrosis. Dig Dis. 2015;33:492–497. - PubMed
-
- Tacke F, Trautwein C. Mechanisms of liver fibrosis resolution. J Hepatol. 2015;63:1038–1039. - PubMed
-
- Schuppan D. Liver fibrosis: Common mechanisms and antifibrotic therapies. Clin Res Hepatol Gastroenterol. 2015;39 Suppl 1:S51–S59. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
