

Prospective Evaluation of Opioid Consumption Following Carpal Tunnel Release Surgery
- PMID: 28082841
- PMCID: PMC5207284
- DOI: 10.1177/1558944716646765
Prospective Evaluation of Opioid Consumption Following Carpal Tunnel Release Surgery
Abstract
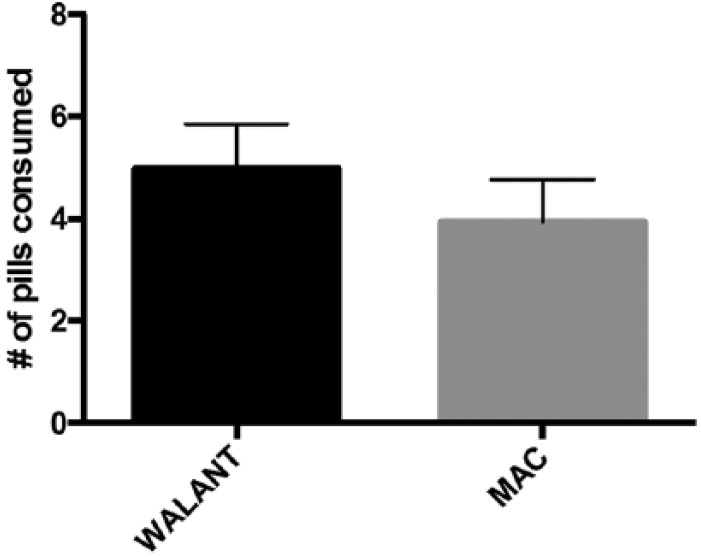
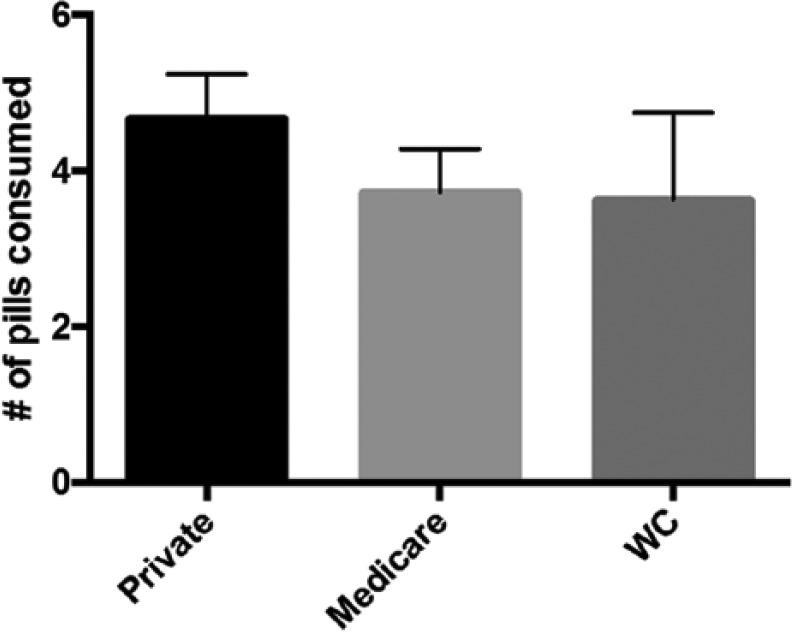
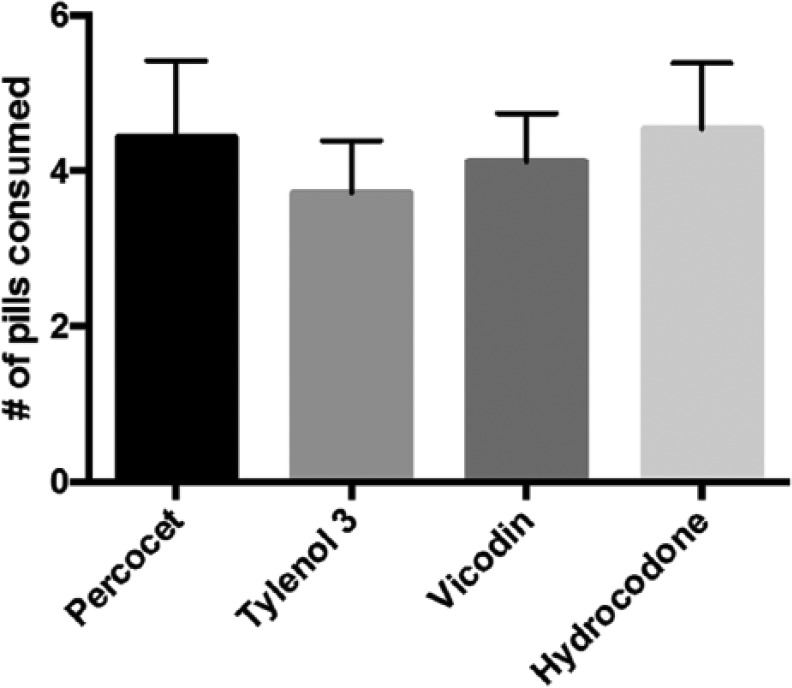
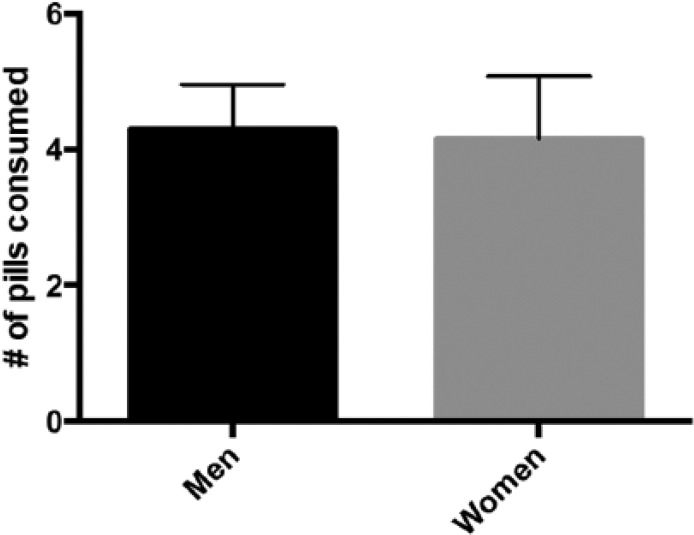
Background: Postoperative pain management and opioid consumption following carpal tunnel release (CTR) surgery may be influenced by many variables. To understand factors affecting opioid consumption, a prospective study was undertaken with the hypothesis that CTR performed under local anesthesia (wide awake local anesthesia with no tourniquet [WALANT]) would result in increased opioid consumption postoperatively compared with cases performed under sedation. Methods: All patients undergoing open CTR surgery were consecutively enrolled over a 6-month period. Information collected included patient demographics, surgical technique, amount and type of narcotic prescribed, number of pills taken, and type of anesthesia. Results: 277 patients were enrolled (56% women, 44% men). On average, 21 pills were prescribed, and 4.3 pills (median = 2) were consumed. There was no difference in consumption between patients who received WALANT (78 cases) versus (198 cases) sedation (4.9 vs 3.9 pills, respectively) (P = .22). There was no difference in opioid consumption based on insurance type (P = .47) or type of narcotic (P = .85). However, more men consumed no opioids (47%) compared with women (36%) (P < .05) and older patients consumed less than younger patients (P < .05). Conclusions: Opioid consumption following CTR is more influenced by age and gender, and less influenced by anesthesia type, insurance type, or the type of opioid prescribed. Many more opioids were prescribed than needed, on an average of 5:1. Many patients, particularly older patients, do not require any opioid analgesia after CTR.
Keywords: carpal tunnel release; narcotic usage; opioid consumption; outpatient surgery; soft tissue procedure.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Alam A, Gomes T, Zheng H, Mamdani MM, Juurlink DN, Bell CM. Long term analgesic use after low risk surgery: a retrospective cohort study. Arch Intern Med. 2012;172:425-430. - PubMed
-
- Cai R, Crane E, Poneleit K, Paulozzi L. Emergency department visits involving nonmedical use of selected prescription drugs—United States, 2004-2008. Morb Mortal Wkly Rep. 2010;59:705-709.
-
- Carroll I, Barkelka P, Wang CK, et al. A pilot cohort study of the determinants of longitudinal opioid use after surgery. Anesth Analg. 2012;115:694-702. - PubMed
-
- Chen L, Hedegaard H, Warner M. QuickStats: Number of Deaths From Poisoning, Drug Poisoning, and Drug Poisoning Involving Opioid Analgesics—United States, 1999-2010. Atlanta, GA: Centers for Disease Control and Prevention; 2013.
-
- Governale L. Outpatient prescription opioid utilization in the U.S., years 2000–2009. Presentation for US Food and Drug Administration; July 22, 2010; Silver Spring, MD http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMateria....
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
