

Prevalence of Diabetes in the 2009 Influenza A (H1N1) and the Middle East Respiratory Syndrome Coronavirus: A Systematic Review and Meta-Analysis
- PMID: 28083520
- PMCID: PMC5206772
- DOI: 10.4081/jphr.2016.733
Prevalence of Diabetes in the 2009 Influenza A (H1N1) and the Middle East Respiratory Syndrome Coronavirus: A Systematic Review and Meta-Analysis
Abstract
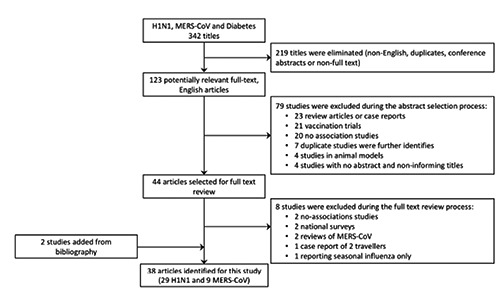
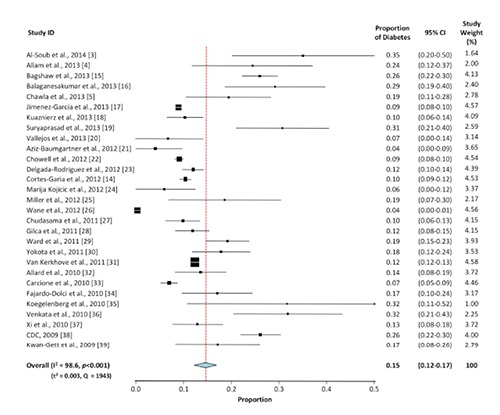
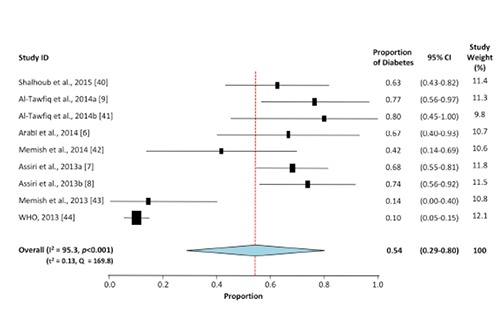
Over the past two decades a number of severe acute respiratory infection outbreaks such as the 2009 influenza A (H1N1) and the Middle East respiratory syndrome coronavirus (MERS-CoV) have emerged and presented a considerable global public health threat. Epidemiologic evidence suggests that diabetic subjects are more susceptible to these conditions. However, the prevalence of diabetes in H1N1 and MERS-CoV has not been systematically described. The aim of this study is to conduct a systematic review and meta-analysis of published reports documenting the prevalence of diabetes in H1N1 and MERS-CoV and compare its frequency in the two viral conditions. Meta-analysis for the proportions of subjects with diabetes was carried out in 29 studies for H1N1 (n=92,948) and 9 for MERS-CoV (n=308). Average age of H1N1 patients (36.2±6.0 years) was significantly younger than that of subjects with MERS-CoV (54.3±7.4 years, P<0.05). Compared to MERS-CoV patients, subjects with H1N1 exhibited 3-fold lower frequency of cardiovascular diseases and 2- and 4-fold higher prevalence of obesity and immunosuppression, respectively. The overall prevalence of diabetes in H1N1 was 14.6% (95% CI: 12.3-17.0%; P<0.001), a 3.6-fold lower than in MERS-CoV (54.4%; 95% CI: 29.4-79.5; P<0.001). The prevalence of diabetes among H1N1 cases from Asia and North America was ~two-fold higher than those from South America and Europe. The prevalence of diabetes in MERS-CoV cases is higher than in H1N1. Regional comparisons suggest that an etiologic role of diabetes in MERS-CoV may exist distinctive from that in H1N1.
Keywords: 2009 influenza A (H1N1); Diabetes mellitus; Systematic Review; the Middle East respiratory syndrome coronavirus (MERS-CoV).
Conflict of interest statement
the authors declare no conflict of interest.
Figures
References
-
- Dawood FS, Iuliano AD, Reed C, et al. Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modeling study. Lancet Infect Dis 2012;12:687-95. - PubMed
-
- World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV). 2015. Available from: http://www.who.int/emergencies/mers-cov/en/ (accessed on October 29, 2015).
-
- Al-Soub H, Ibrahim AS, Al-Maslamani M, et al. Epidemiology, risk factors, clinical features, and outcome of adult patients with severe pandemic A/H1N1/2009 influenza in Qatar: a retrospective study. Infect Dis Clin Pract 2014;22:339-43.
-
- Allam RR, Murhekar MV, Tadi GP, Udaragudi PR. Descriptive epidemiology of novel influenza A (H1N1), Andhra Pradesh 2009-2010. Ind J Pub Health 2013;57:161-5. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
