

Practical use of visual medial temporal lobe atrophy cut-off scores in Alzheimer's disease: Validation in a large memory clinic population
- PMID: 28083697
- PMCID: PMC5491609
- DOI: 10.1007/s00330-016-4726-3
Practical use of visual medial temporal lobe atrophy cut-off scores in Alzheimer's disease: Validation in a large memory clinic population
Abstract
Objective: To provide age-specific medial temporal lobe atrophy (MTA) cut-off scores for routine clinical practice as marker for Alzheimer's disease (AD).
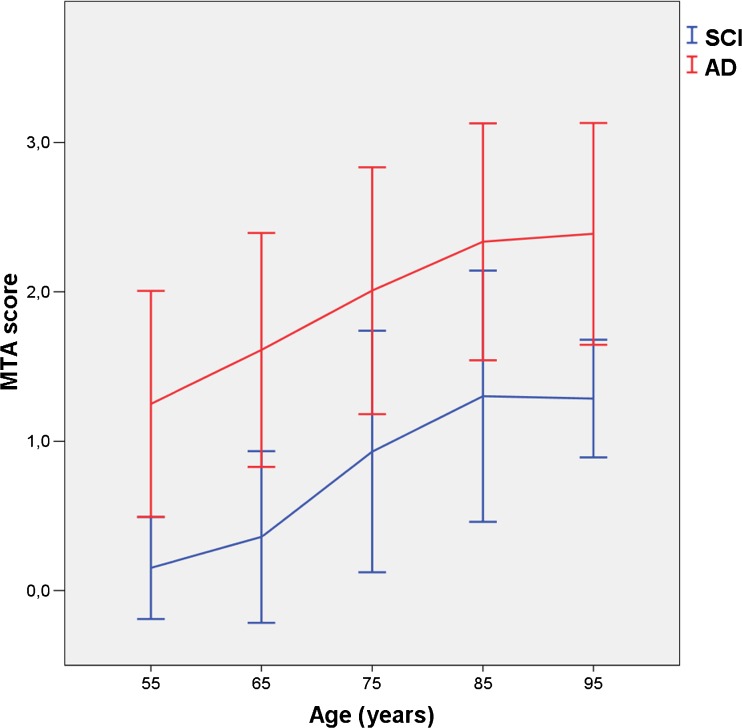
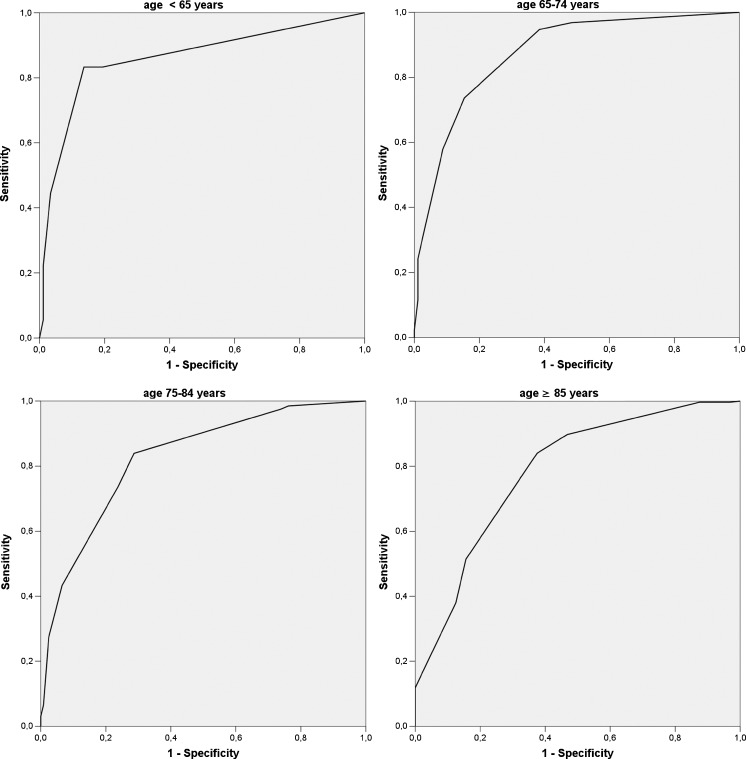
Methods: Patients with AD (n = 832, mean age 81.8 years) were compared with patients with subjective cognitive impairment (n = 333, mean age 71.8 years) in a large single-centre memory clinic. Mean of right and left MTA scores was determined with visual rating (Scheltens scale) using CT (0, no atrophy to 4, severe atrophy). Relationships between age and MTA scores were analysed with regression analysis. For various MTA cut-off scores, decade-specific sensitivity and specificity and area under the curve (AUC) values, computed with receiver operator characteristic curves, were determined.
Results: MTA strongly increased with age in both groups to a similar degree. Optimal MTA cut-off values for the age ranges <65, 65-74, 75-84 and ≥85 were: ≥1.0, ≥1.5, ≥ 2.0 and ≥2.0. Corresponding values of sensitivity and specificity were 83.3% and 86.4%; 73.7% and 84.6%; 73.7% and 76.2%; and 84.0% and 62.5%.
Conclusion: From this large unique memory clinic cohort we suggest decade-specific MTA cut-off scores for clinical use. After age 85 years, however, the practical usefulness of the MTA cut-off is limited.
Key points: • We suggest decade-specific MTA cut-off scores for AD. • MTA cut-off after the age of 85 years has limited use. • CT is feasible and accurate for visual MTA rating.
Keywords: Alzheimer’s disease; Clinical practice; Computed tomography; Diagnostic imaging; Temporal lobe.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is Philip Scheltens.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Funding
This study has received funding by the Tergooi Academy, Tergooi Hospital.
Statistics and biometry
One of the authors has significant statistical expertise.
Ethical approval
Institutional Review Board approval was obtained.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Methodology
Retrospective, cross-sectional study, performed at one institution.
Figures
References
-
- McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:263–269. doi: 10.1016/j.jalz.2011.03.005. - DOI - PMC - PubMed
-
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:270–279. doi: 10.1016/j.jalz.2011.03.008. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
