

Can Multistate Modeling of Local Recurrence, Distant Metastasis, and Death Improve the Prediction of Outcome in Patients With Soft Tissue Sarcomas?
- PMID: 28083752
- PMCID: PMC5384928
- DOI: 10.1007/s11999-017-5232-x
Can Multistate Modeling of Local Recurrence, Distant Metastasis, and Death Improve the Prediction of Outcome in Patients With Soft Tissue Sarcomas?
Abstract
Background: Exploration of the complex relationship between prognostic indicators such as tumor grade and size and clinical outcomes such as local recurrence and distant metastasis in patients with cancer is crucial to guide treatment decisions. However, in patients with soft tissue sarcoma, there are many gaps in our understanding of this relationship. Multistate analysis may help us in gaining a comprehensive understanding of risk factor-outcome relationships in soft tissue sarcoma, because this methodology can integrate multiple risk factors and clinical endpoints into a single statistical model. To our knowledge, no study of this kind has been performed before in patients with soft tissue sarcoma.
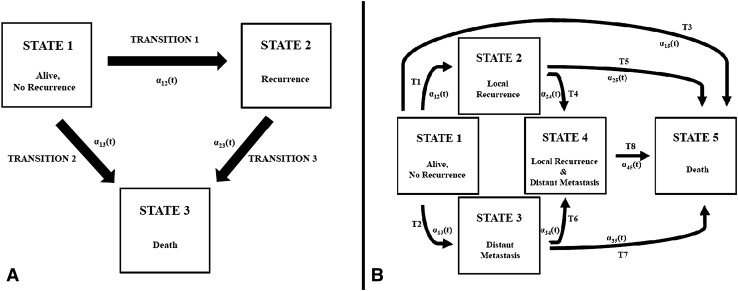
Questions/purposes: We implemented a multistate model of localized soft tissue sarcoma to statistically evaluate the relationship among baseline risk factors, recurrence, and death in patients with localized soft tissue sarcoma undergoing curative surgery.
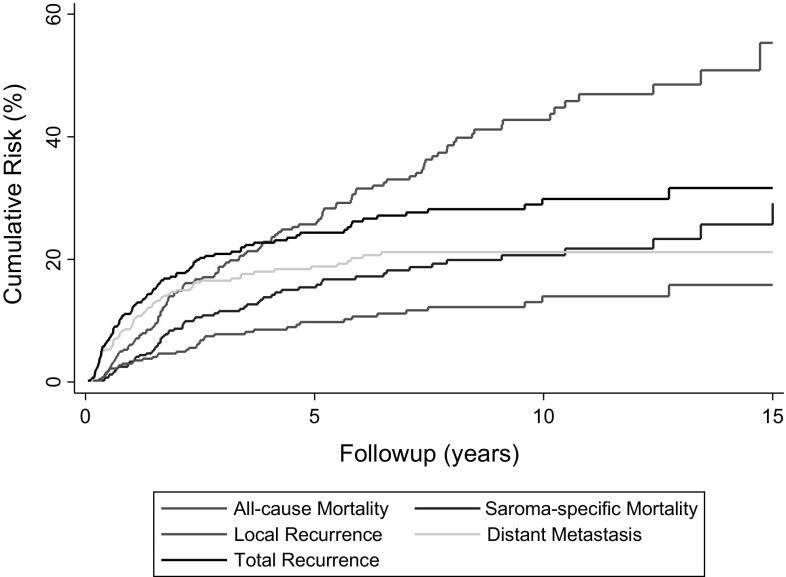
Methods: Between 1998 and 2015, our center treated 539 patients for localized soft tissue sarcoma with surgery as curative intent. Of those, 96 patients (18%) were not included in this single-center retrospective study owing to missing baseline histopathology data (n = 3), not yet observed followup (n = 80), or because a neoadjuvant treatment approach in the presence of synchronous distant metastasis was used (n = 13), leaving 443 patients (82%) for the current analysis, of which 40 were lost to followup during the first year after surgery. All patients had tumors of the stages I to III according to the American Joint Committee on Cancer Stages. The median age of the patients was 62 years (range, 16-96 years), and 217 patients (49%) were female. Three hundred-forty-six patients (78%) had tumors of high grade (Grades 2 and 3), and 310 (70%) tumors were greater than 5 cm in maximum diameter. Patients who had died during the first year of followup were included in this analysis. Median followup for the 443 study patients was 6 years, with 84%, 52%, and 23% of patients being followed for more than 1, 5, and 10 years, respectively. The 15-year cumulative incidences of local recurrence, distant metastasis, and death from any cause, using a competing risk analysis, were 16% (95% CI, 11%-22%), 21% (95% CI, 17%-26%), and 55% (95% CI, 44%-67%), respectively. Wide resection with a margin of 1 mm was the preferred treatment for all patients, except for those with Grade 1 liposarcoma where a marginal resection was considered adequate. Multistate models were implemented with the mstate library in R.
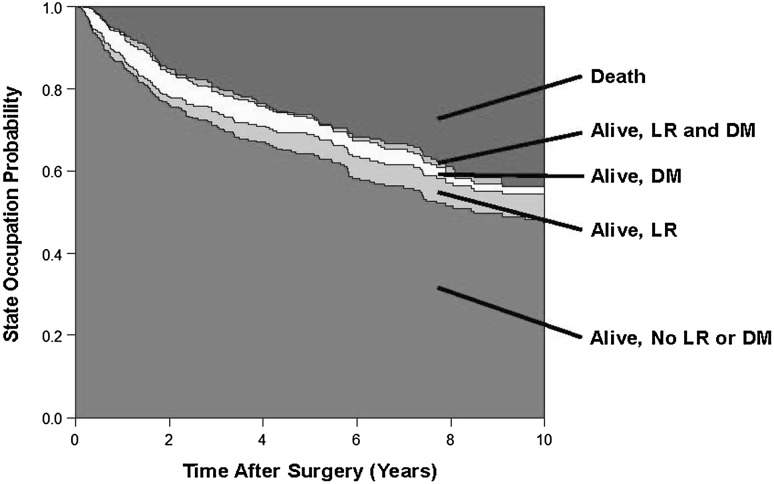
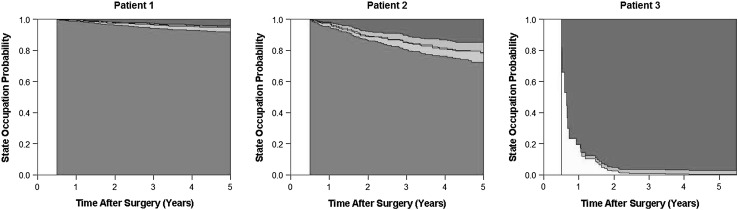
Results: In multistate analysis, patients who experienced a local recurrence were more likely to have distant metastasis develop (hazard ratio [HR] = 8.4; 95% CI, 4.3-16.5; p < 0.001), and to die (HR = 3.4; 95% CI, 2.1-5.6; p < 0.001). The occurrence of distant metastasis was associated with a strong increase in the risk of death (HR = 12.6; 95% CI, 8.7-18.3; p < 0.001). Distant metastasis occurring after a long tumor-free interval was not associated with a more-favorable prognosis with respect to mortality than distant metastasis occurring early after surgery (estimated relative decrease in the adverse effect of distant metastasis on mortality for 1-year delay in the occurrence of distant metastasis = 0.9; 95% CI, 0.7-1.1; p = 0.28). High-grade histology (Grades 2 and 3) was associated with a higher risk of overall recurrence (defined as a composite of local recurrence and distant metastasis, HR = 3.8; 95% CI, 1.8-7.8; p = 0.0003) and a higher risk of death after recurrence developed (HR = 4.4; 95% CI, 1.1-18.2; p = 0.04). Finally, the multistate model predicted distinct outcome patterns depending on baseline covariates and how long a patient has remained free from recurrence after surgery.
Conclusions: In patients with localized soft tissue sarcoma undergoing resection, the occurrence of local recurrence and distant metastasis contributes to a dramatically impaired long-term survival outcome. Local recurrences are a substantial risk factor for distant metastasis. Multistate modeling is a very powerful approach for analysis of sarcoma cohorts, and may be used in the future to obtain highly personalized, dynamic predictions of outcomes in patients with localized soft tissue sarcoma.
Level of evidence: Level III, therapeutic study.
Figures
Comment in
-
CORR Insights®: Can Multistate Modeling of Local Recurrence, Distant Metastasis, and Death Improve the Prediction of Outcome in Patients With Soft Tissue Sarcomas?Clin Orthop Relat Res. 2017 May;475(5):1436-1438. doi: 10.1007/s11999-017-5295-8. Epub 2017 Feb 27. Clin Orthop Relat Res. 2017. PMID: 28243974 Free PMC article. No abstract available.
References
-
- Callegaro D, Miceli R, Bonvalot S, Ferguson P, Strauss DC, Levy A, Griffin A, Hayes AJ, Stacchiotti S, Pechoux CL, Smith MJ, Fiore M, Dei Tos AP, Smith HG, Mariani L, Wunder JS, Pollock RE, Casali PG, Gronchi A. Development and external validation of two nomograms to predict overall survival and occurrence of distant metastases in adults after surgical resection of localised soft-tissue sarcomas of the extremities: a retrospective analysis. Lancet Oncol. 2016;17:671–680. doi: 10.1016/S1470-2045(16)00010-3. - DOI - PubMed
-
- ESMO/European Sarcoma Neteork Working Group. Soft tissue and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(suppl 3):iii102-112. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
