

Diabetes and Tuberculosis
- PMID: 28084206
- PMCID: PMC5240796
- DOI: 10.1128/microbiolspec.TNMI7-0023-2016
Diabetes and Tuberculosis
Abstract
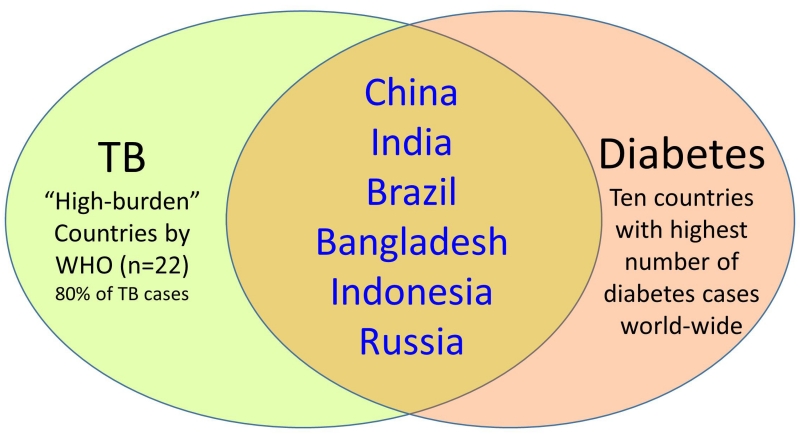
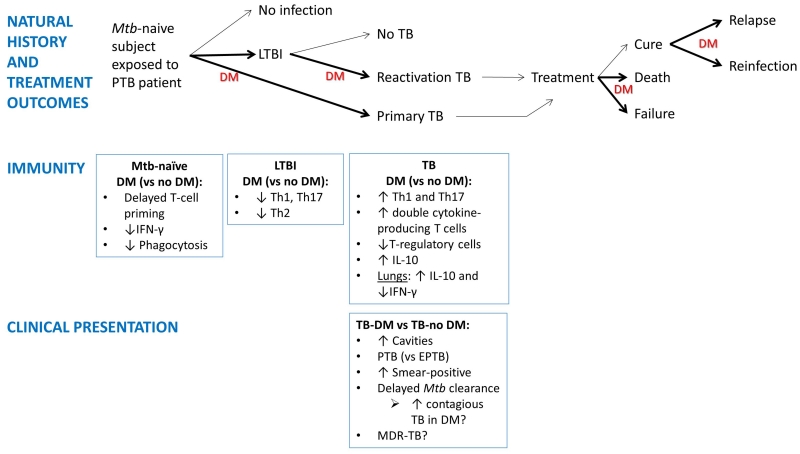
The increase in type 2 diabetes mellitus (DM) patients in countries where tuberculosis (TB) is also endemic has led to the reemerging importance of DM as a risk factor for TB. DM causes a 3-fold increase in TB risk and a 2-fold increase in adverse TB treatment outcomes. Given the sheer numbers of DM patients worldwide, there are now more TB patients with TB-DM comorbidity than TB-HIV coinfection. There is an urgent need to implement strategies for TB prevention and control among the millions of DM patients exposed to Mycobacterium tuberculosis. This chapter summarizes the current epidemiological, clinical, and immunological knowledge on TB and DM and their clinical and public health implications. These include the underlying mechanisms for TB risk in DM patients and their clinical and sociodemographic characteristics that distinguish them from TB patients without DM. TB-DM comorbidity is posing a new challenge for integrating the short-term care for TB with the long-term care for DM, particularly in low- and middle-income countries.
Figures
References
-
- Ottmani SE, Murray MB, Jeon CY, Baker MA, Kapur A, Lonnroth K, Harries AD. Consultation meeting on tuberculosis and diabetes mellitus: meeting summary and recommendations. Int J Tuberc Lung Dis. 2010;14:1513–1517. - PubMed
-
- Ronacher K, Joosten SA, van Crevel R, Dockrell HM, Walzl G, Ottenhoff TH. Acquired immunodeficiencies and tuberculosis: focus on HIV/AIDS and diabetes mellitus. Immunol Rev. 2015;264:121–137. - PubMed
-
- Morton R. Phthisiologia, Or a Treatise of Consumptions. London, England: 1694.
-
- Boucot KR, Dillon ES, Cooper DA, Meier P, Richardson R. Tuberculosis among diabetics: the Philadelphia survey. Am Rev Tuberc. 1952;65:1–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
