

Improvement of Uveal and Capsular Biocompatibility of Hydrophobic Acrylic Intraocular Lens by Surface Grafting with 2-Methacryloyloxyethyl Phosphorylcholine-Methacrylic Acid Copolymer
- PMID: 28084469
- PMCID: PMC5234006
- DOI: 10.1038/srep40462
Improvement of Uveal and Capsular Biocompatibility of Hydrophobic Acrylic Intraocular Lens by Surface Grafting with 2-Methacryloyloxyethyl Phosphorylcholine-Methacrylic Acid Copolymer
Abstract
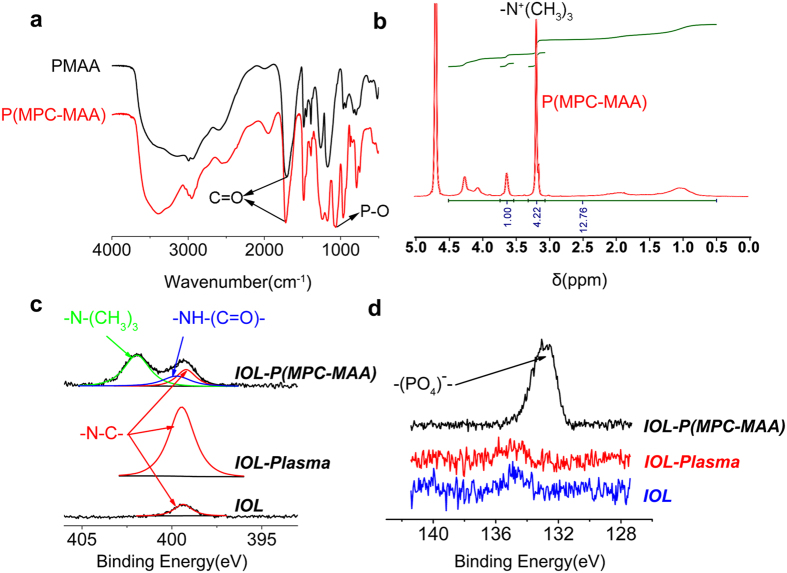
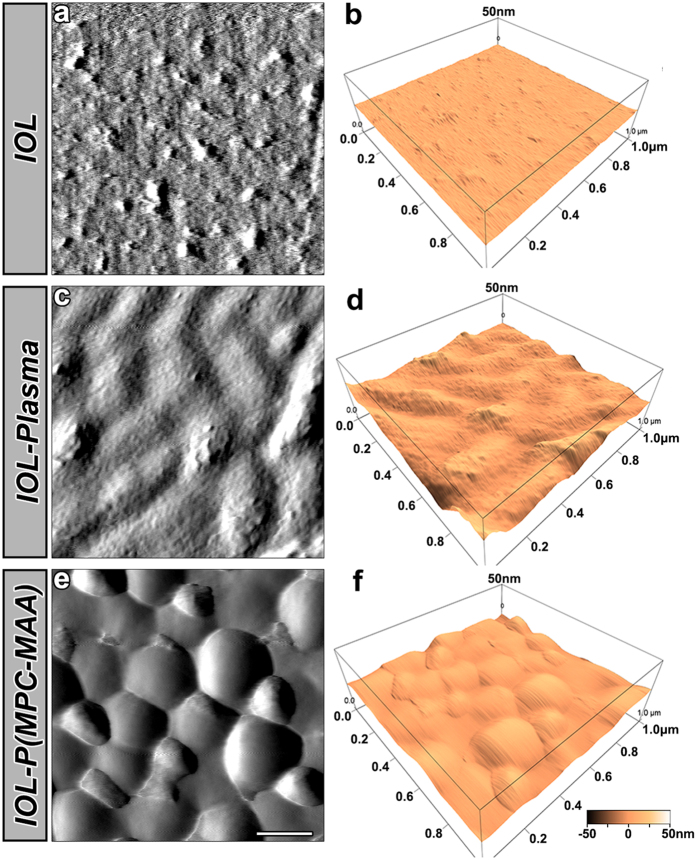
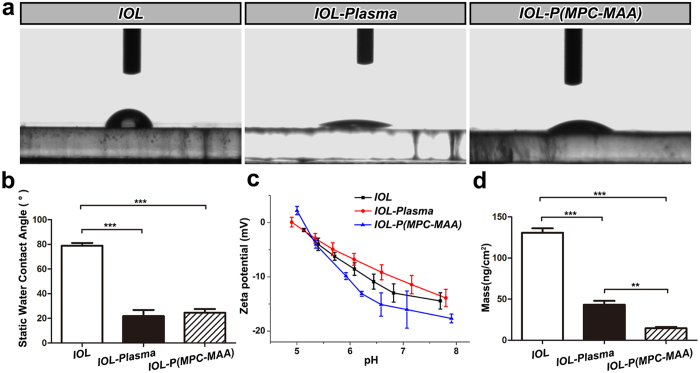
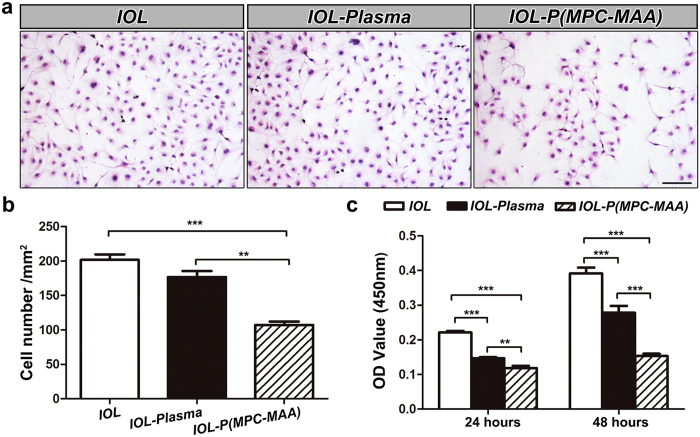
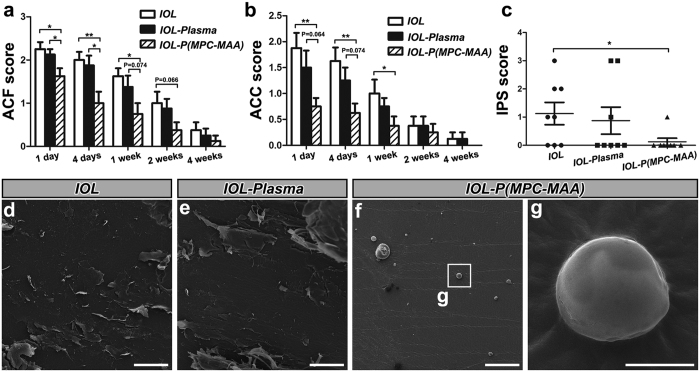
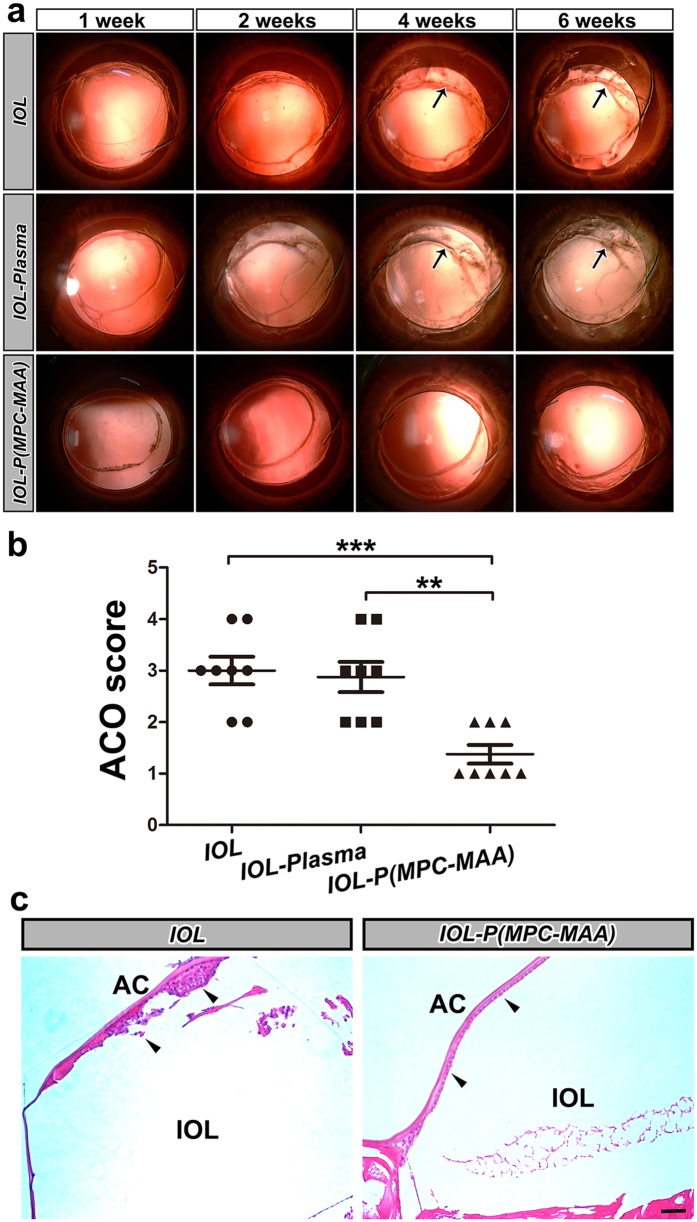
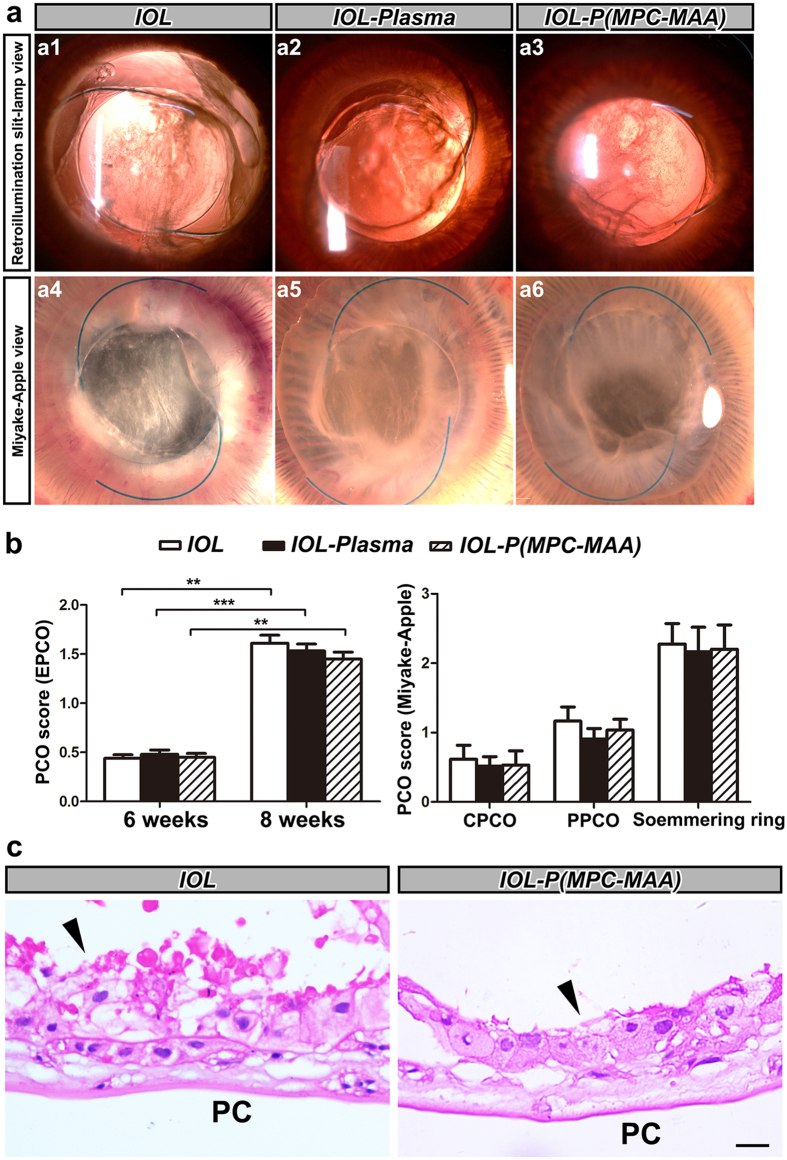
Biocompatibility of intraocular lens (IOL) is critical to vision reconstruction after cataract surgery. Foldable hydrophobic acrylic IOL is vulnerable to the adhesion of extracellular matrix proteins and cells, leading to increased incidence of postoperative inflammation and capsule opacification. To increase IOL biocompatibility, we synthesized a hydrophilic copolymer P(MPC-MAA) and grafted the copolymer onto the surface of IOL through air plasma treatment. X-ray photoelectron spectroscopy, atomic force microscopy and static water contact angle were used to characterize chemical changes, topography and hydrophilicity of the IOL surface, respectively. Quartz crystal microbalance with dissipation (QCM-D) showed that P(MPC-MAA) modified IOLs were resistant to protein adsorption. Moreover, P(MPC-MAA) modification inhibited adhesion and proliferation of lens epithelial cells (LECs) in vitro. To analyze uveal and capsular biocompatibility in vivo, we implanted the P(MPC-MAA) modified IOLs into rabbits after phacoemulsification. P(MPC-MAA) modification significantly reduced postoperative inflammation and anterior capsule opacification (ACO), and did not affect posterior capsule opacification (PCO). Collectively, our study suggests that surface modification by P(MPC-MAA) can significantly improve uveal and capsular biocompatibility of hydrophobic acrylic IOL, which could potentially benefit patients with blood-aqueous barrier damage.
Figures
References
-
- Wang G. et al. In vivo implantation of hydrophobic acrylic intraocular lenses with surface modification. Eye Sci 28, 176–179 (2013). - PubMed
-
- Abela-Formanek C., Amon M., Kahraman G., Schauersberger J. & Dunavoelgyi R. Biocompatibility of hydrophilic acrylic, hydrophobic acrylic, and silicone intraocular lenses in eyes with uveitis having cataract surgery: Long-term follow-up. J Cataract Refract Surg 37, 104–112, doi: 10.1016/j.jcrs.2010.07.038 (2011). - DOI - PubMed
-
- Richter-Mueksch S. et al. Uveal and capsular biocompatibility after implantation of sharp-edged hydrophilic acrylic, hydrophobic acrylic, and silicone intraocular lenses in eyes with pseudoexfoliation syndrome. J Cataract Refract Surg 33, 1414–1418, doi: 10.1016/j.jcrs.2007.05.009 (2007). - DOI - PubMed
-
- Saika S., Miyamoto T. & Ohnishi Y. Histology of anterior capsule opacification with a polyHEMA/HOHEXMA hydrophilic hydrogel intraocular lens compared to poly(methyl methacrylate), silicone, and acrylic lenses. J Cataract Refract Surg 29, 1198–1203 (2003). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
