

Total kidney and liver volume is a major risk factor for malnutrition in ambulatory patients with autosomal dominant polycystic kidney disease
- PMID: 28088190
- PMCID: PMC5237538
- DOI: 10.1186/s12882-016-0434-0
Total kidney and liver volume is a major risk factor for malnutrition in ambulatory patients with autosomal dominant polycystic kidney disease
Abstract
Background: In patients with autosomal dominant polycystic kidney disease (ADPKD), malnutrition may develop as renal function declines and the abdominal organs become enlarged. We investigated the relationship of intra-abdominal mass with nutritional status.
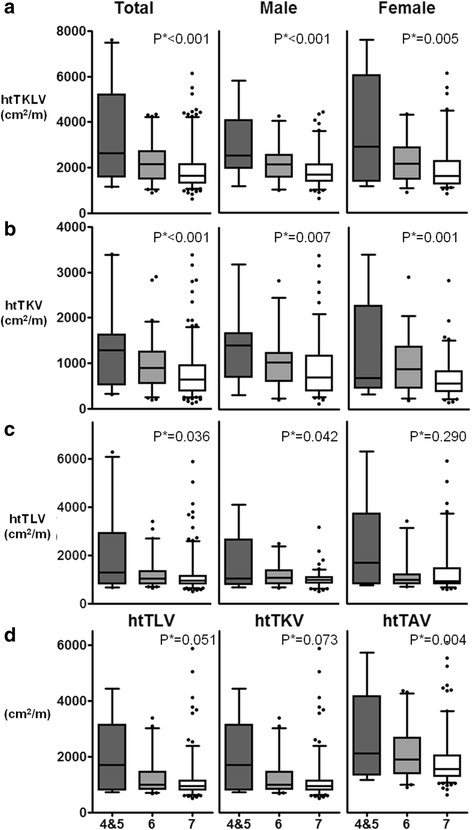
Methods: This cross-sectional study was performed at a tertiary hospital outpatient clinic. Anthropometric and laboratory data including serum creatinine, albumin, and cholesterol were collected, and kidney and liver volumes were measured. Total kidney and liver volume was defined as the sum of the kidney and liver volumes and adjusted by height (htTKLV). Nutritional status was evaluated by using modified subjective global assessment (SGA).
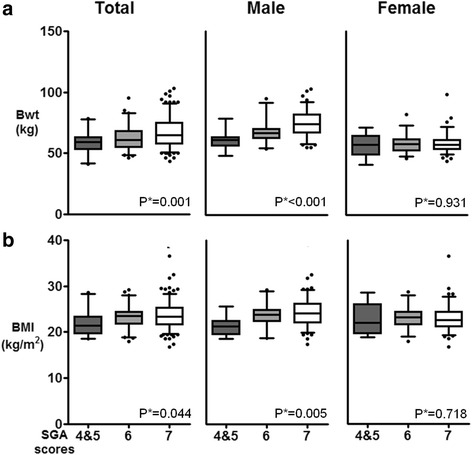
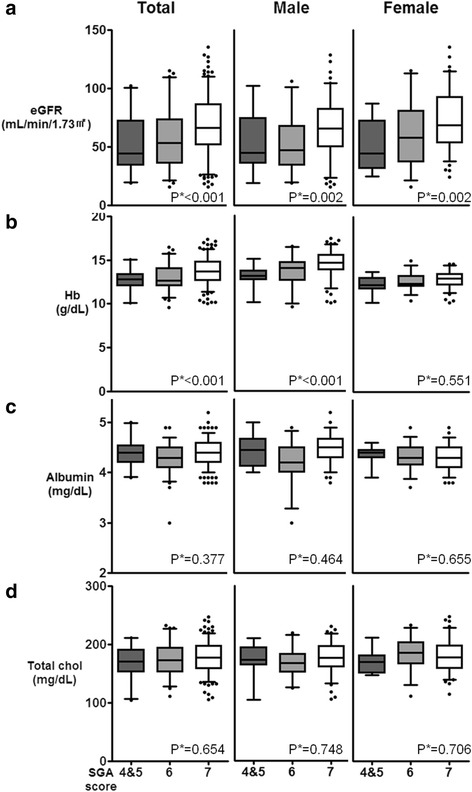
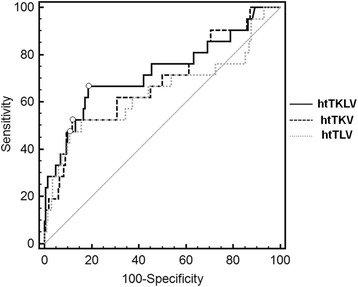
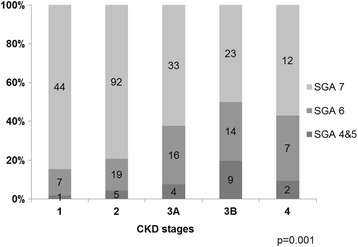
Results: In a total of 288 patients (47.9% female), the mean age was 48.3 ± 12.2 years and the mean estimated glomerular filtration rate (eGFR) was 65.3 ± 25.3 mL/min/1.73 m2. Of these patients, 21 (7.3%) were mildly to moderately malnourished (SGA score of 4 and 5) and 63 (21.7%) were at risk of malnutrition (SGA score of 6). Overall, patients with or at risk of malnutrition were older, had a lower body mass index, lower hemoglobin levels, and poorer renal function compared to the well-nourished group. However, statistically significant differences in these parameters were not observed in female patients, except for eGFR. In contrast, a higher htTKLV correlated with a lower SGA score, even in subjects with an eGFR ≥45 mL/min/1.73 m2. Subjects with an htTKLV ≥2340 mL/m showed an 8.7-fold higher risk of malnutrition, after adjusting for age, hemoglobin, and eGFR.
Conclusions: Nutritional risk was detected in 30% of ambulatory ADPKD patients with relatively good renal function. Intra-abdominal organomegaly was related to nutritional status independently from renal function deterioration.
Keywords: Autosomal-dominant polycystic kidney disease; Chronic kidney disease; Gender; Malnutrition; Polycystic liver disease.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
