

More Use of Peritoneal Dialysis Gives Significant Savings: A Systematic Review and Health Economic Decision Model
- PMID: 28090226
- PMCID: PMC5215014
- DOI: 10.14740/jocmr2817w
More Use of Peritoneal Dialysis Gives Significant Savings: A Systematic Review and Health Economic Decision Model
Abstract
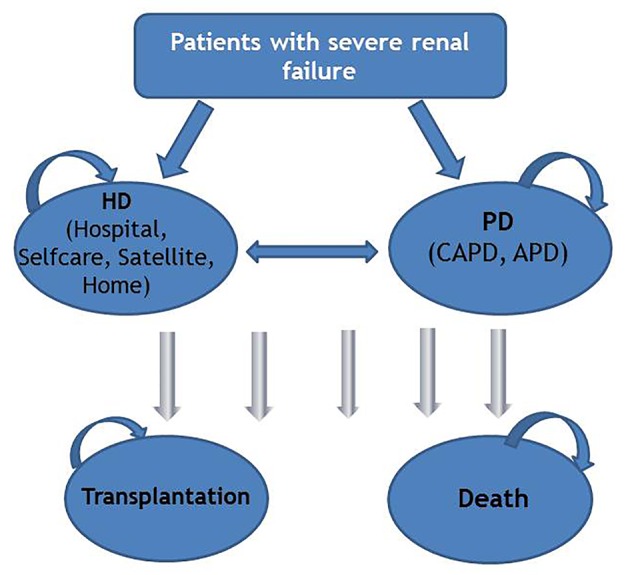
Background: Patients with end-stage renal disease (ESRD) are in need of renal replacement therapy as dialysis and/or transplantation. The prevalence of ESRD and, thus, the need for dialysis are constantly growing. The dialysis modalities are either peritoneal performed at home or hemodialysis (HD) performed in-center (hospital or satellite) or home. We examined effectiveness and cost-effectiveness of HD performed at different locations (hospital, satellite, and home) and peritoneal dialysis (PD) at home in the Norwegian setting.
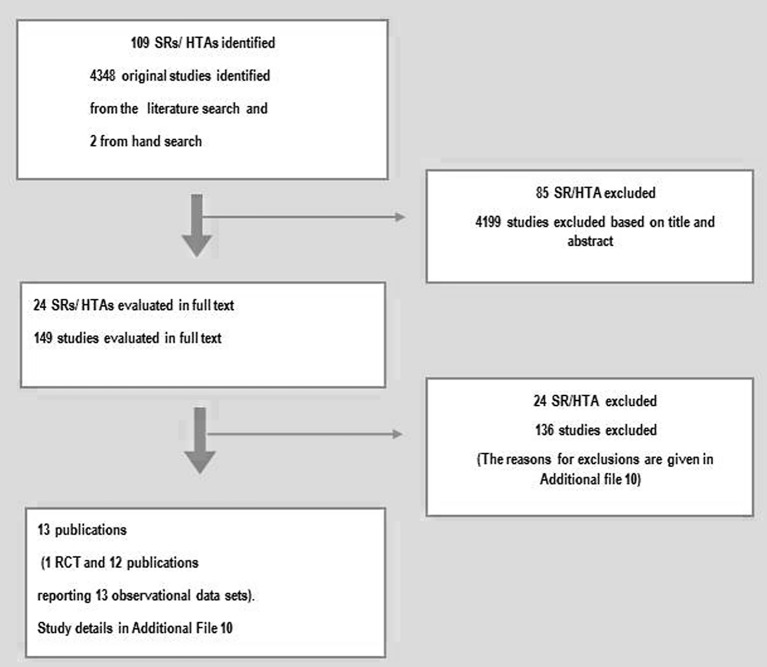
Methods: We conducted a systematic review for patients above 18 years with end-stage renal failure requiring dialysis in several databases and performed several meta-analyses of existing literature. Mortality and major complications that required were our main clinical outcomes. The quality of the evidence for each outcome was evaluated using GRADE. Cost-effectiveness was assessed by developing a probabilistic Markov model. The analysis was carried out from a societal perspective, and effects were expressed in quality-adjusted life-years. Uncertainties in the base-case parameter values were explored with a probabilistic sensitivity analysis. Scenario analyses were conducted by increasing the proportion of patients receiving PD with a corresponding reduction in HD patients in-center both for Norway and Europian Union. We assumed an annual growth rate of 4% in the number of dialysis patients, and a relative distribution between PD and HD in-center of 30% and 70%, respectively.
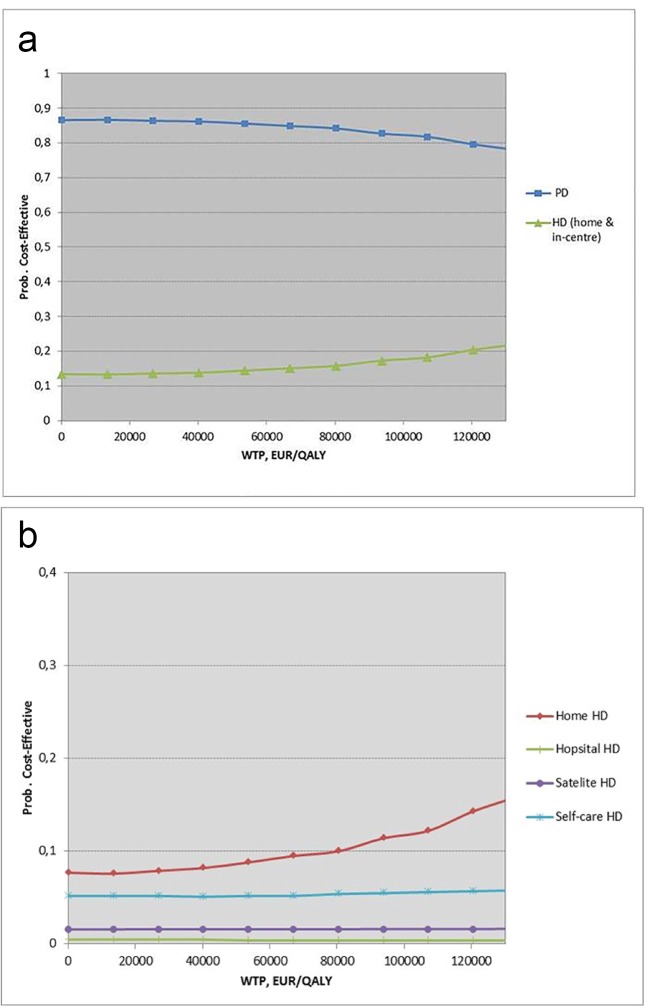
Results: From a societal perspective and over a 5-year time horizon, PD was the most cost-effective dialysis alternative. We found no significant difference in mortality between peritoneal and HD modalities. Our scenario analyses showed that a shift toward more patients on PD (as a first choice) with a corresponding reduction in HD in-center gave a saving over a 5-year period of 32 and 10,623 million EURO, respectively, for Norway and the European Union.
Conclusions: PD was the most cost-effective dialysis alternative and was comparable with HD regarding efficacy outcomes. There are significant saving potentials if more end-stage renal patients are started on PD instead of HD.
Keywords: Dialysis; Health economics; Hemodialysis; Peritoneal.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources