

Classifying thoracolumbar fractures: role of quantitative imaging
- PMID: 28090452
- PMCID: PMC5219967
- DOI: 10.21037/qims.2016.12.04
Classifying thoracolumbar fractures: role of quantitative imaging
Abstract
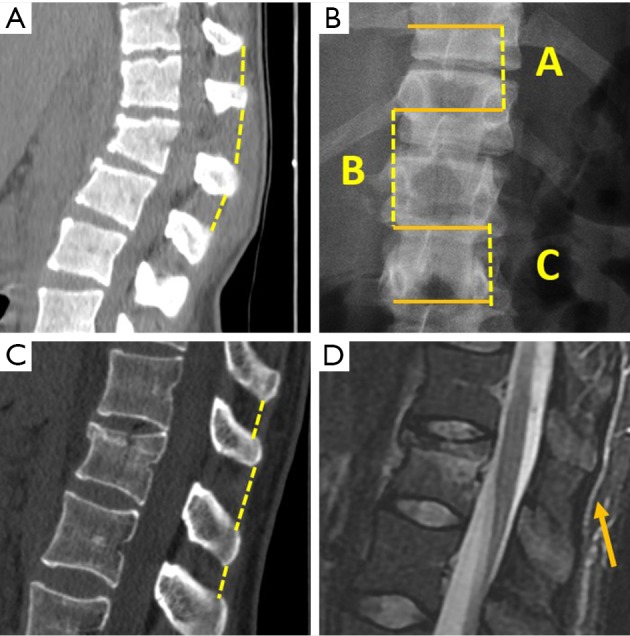
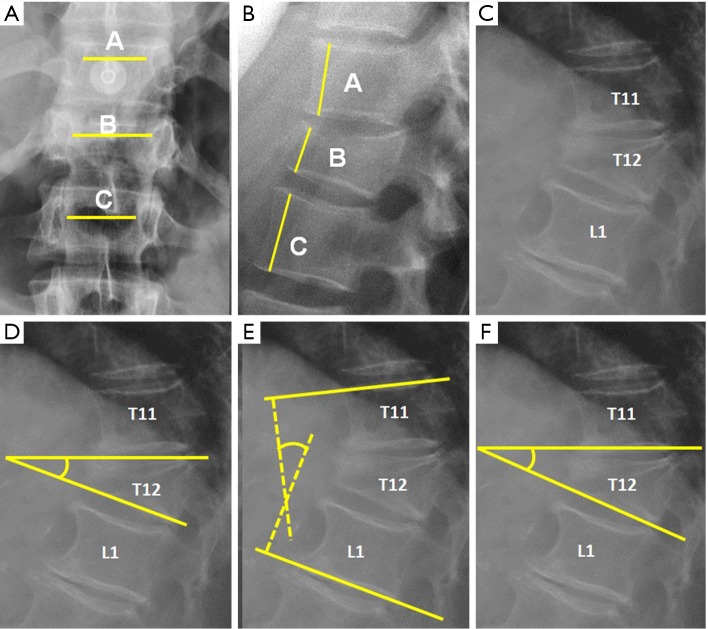
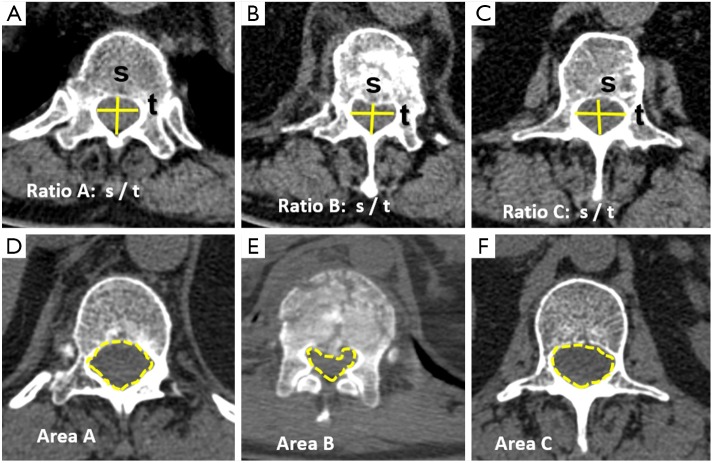
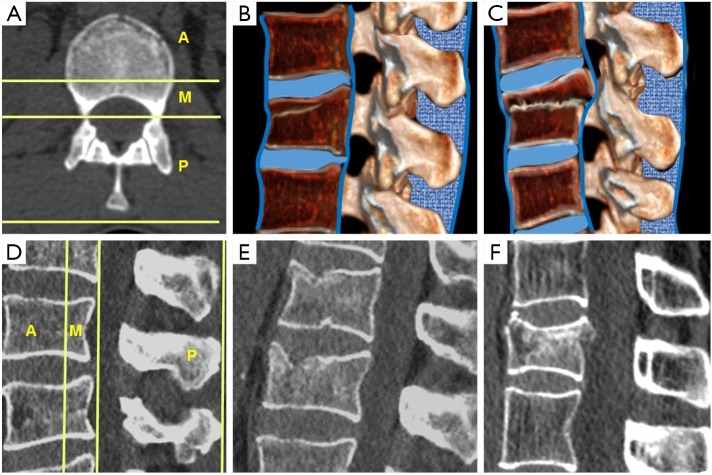
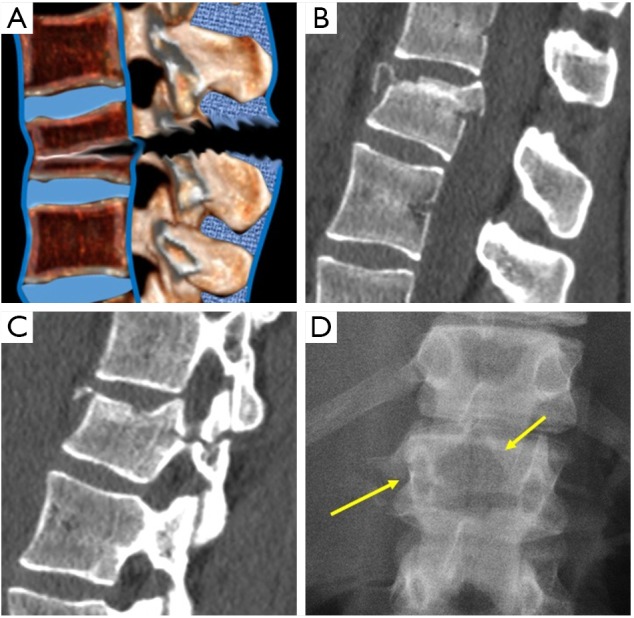
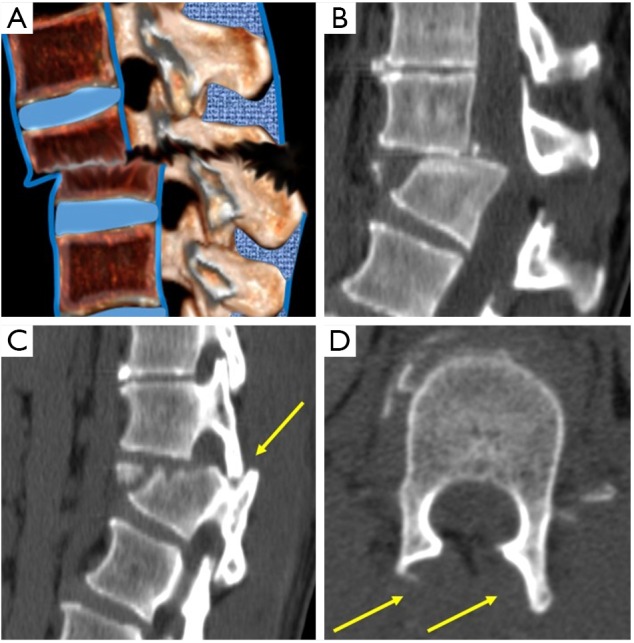
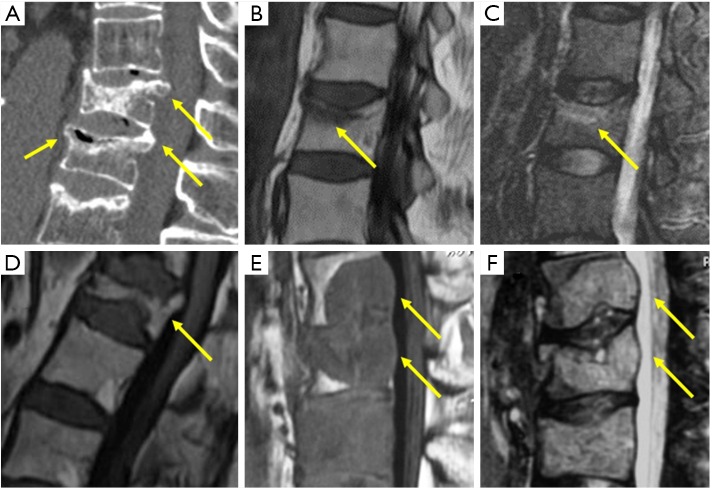
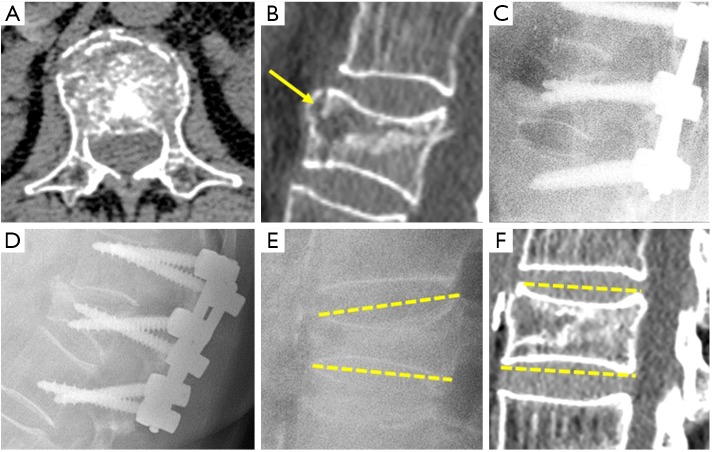
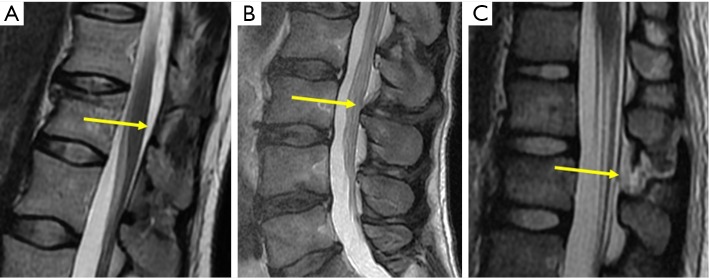
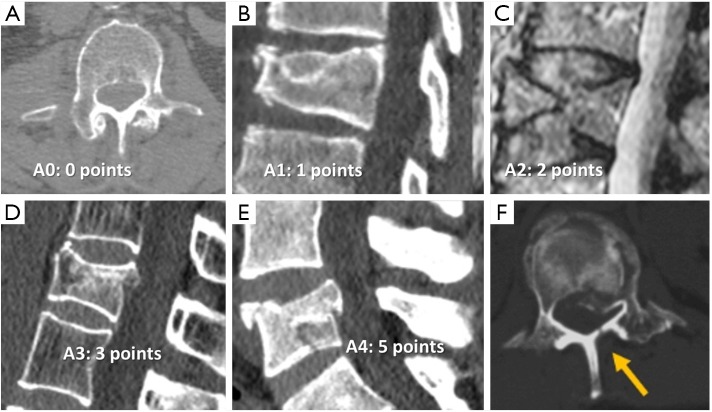
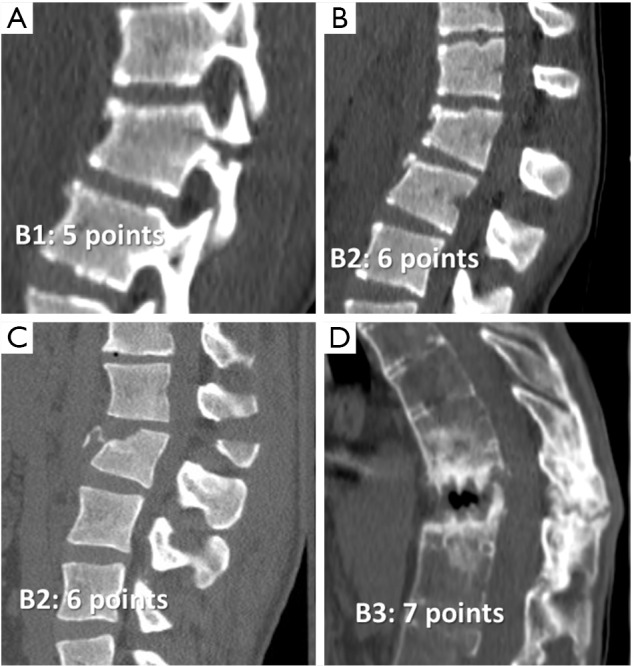
This article describes different types of vertebral fractures that affect the thoracolumbar spine and the most relevant contributions of the different classification systems to vertebral fracture management. The vertebral fractures types are based on the three columns model of Denis that includes compression, burst, flexion-distraction and fracture-dislocation types. The most recent classifications systems of these types of fractures are reviewed, including the Thoracolumbar Injury Classification and Severity score (TLICS) and the Arbeitsgemeinschaft für Osteosynthesefragen Spine Thoracolumbar Injury Classification and Severity score (AOSpine-TLICS). Correct classification requires a quantitative imaging approach in which several measurements determine TLICS or AOSpine-TLICS grade. If the TLICS score is greater than 4, or the AOSpine-TLICS is greater than 5, surgical management is indicated. In this review, the most important imaging findings and measurements on radiography, multidetector computed tomography (MDCT) and magnetic resonance imaging (MRI) are described. These include degree of vertebral wedging and percentage of vertebral height loss in compression fractures, degree of interpedicular distance widening and spinal canal stenosis in burst fractures, and the degree of vertebral translation or interspinous widening in more severe fractures types, such as flexion-distraction and fracture-dislocation. These findings and measurements are illustrated with schemes and cases of our archives in a didactic way.
Keywords: Vertebral fractures; computed tomography; plain radiography; spinal injuries; thoracolumbar trauma.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- DeWald RL. Burst fractures of the thoracic and lumbar spine. Clin Orthop Relat Res 1984;189:150-61. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources