

Functional deficits induced by cortical microinfarcts
- PMID: 28090802
- PMCID: PMC5669342
- DOI: 10.1177/0271678X16685573
Functional deficits induced by cortical microinfarcts
Abstract
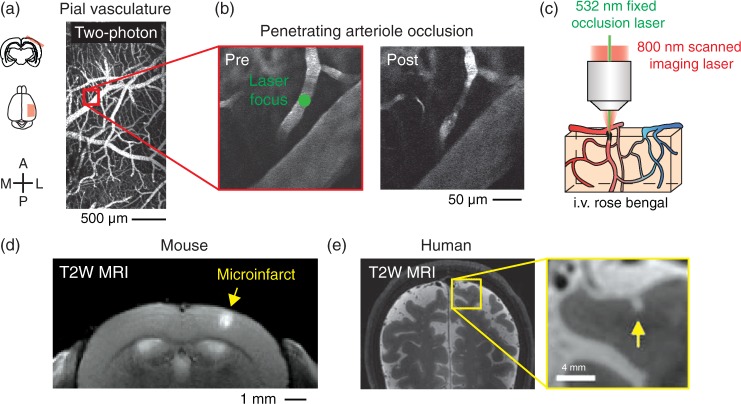
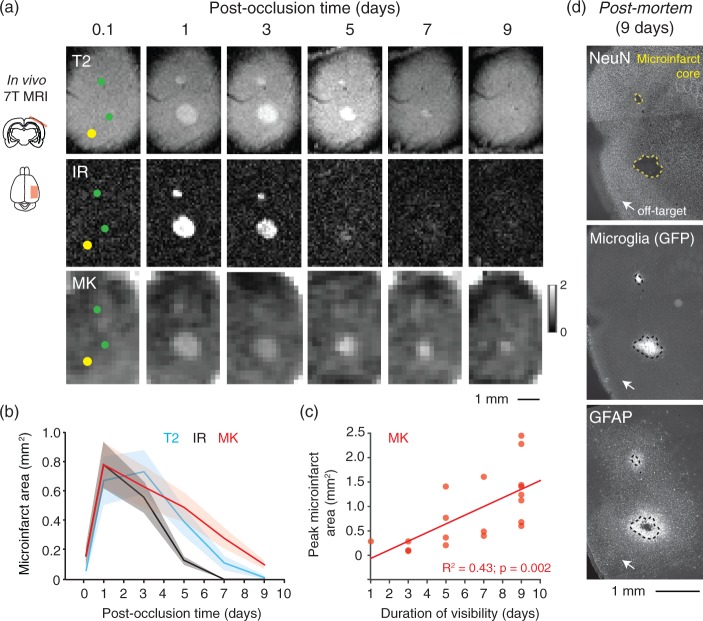
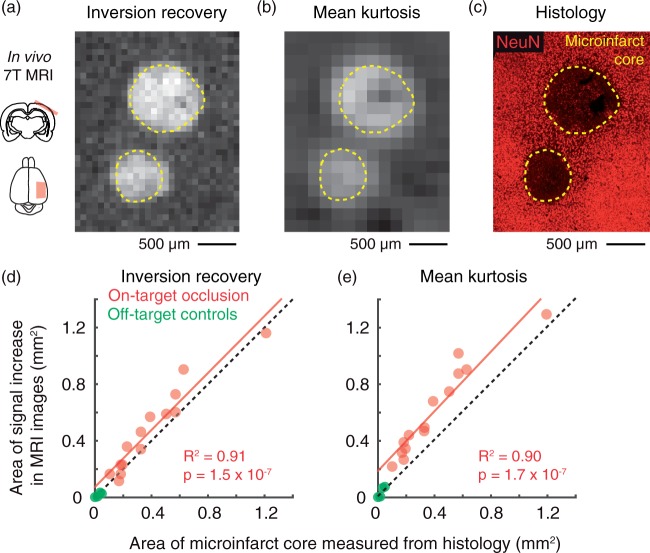
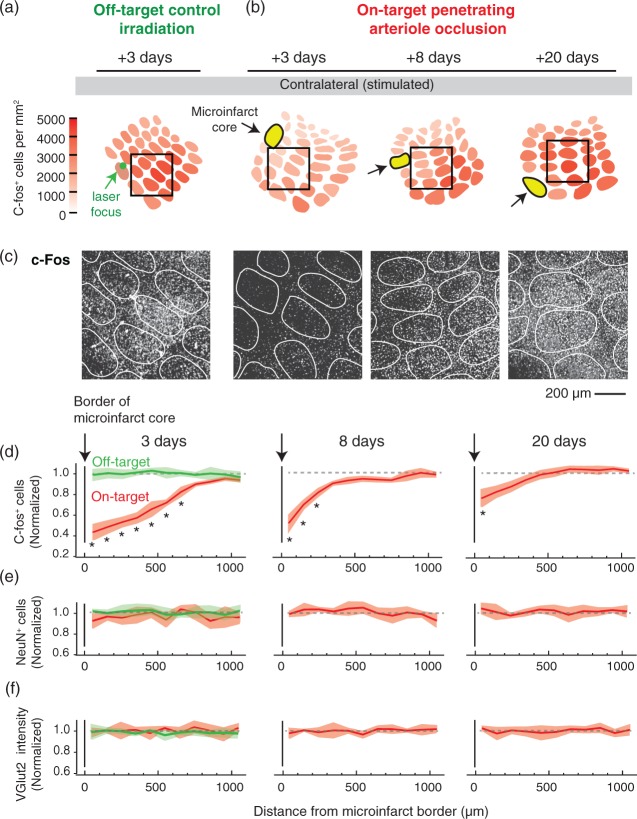
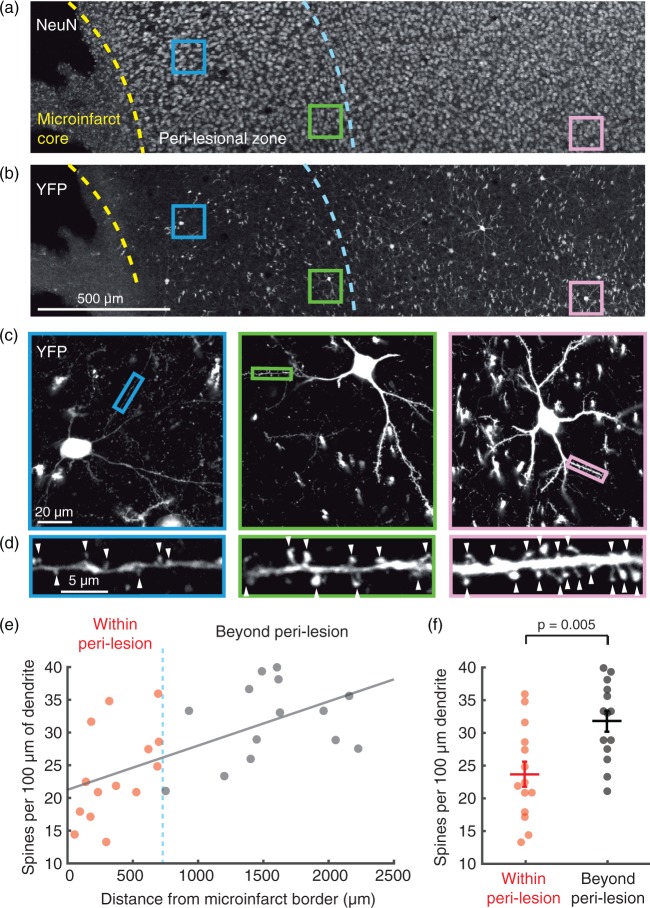
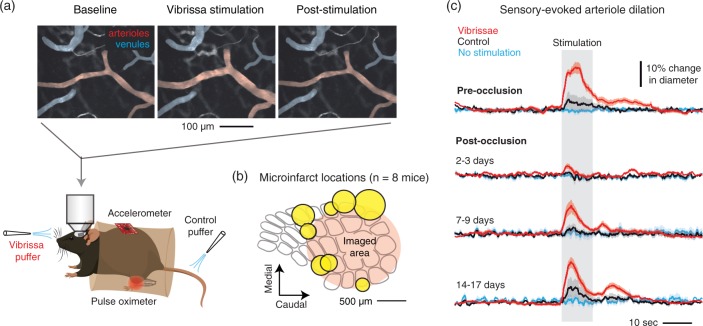
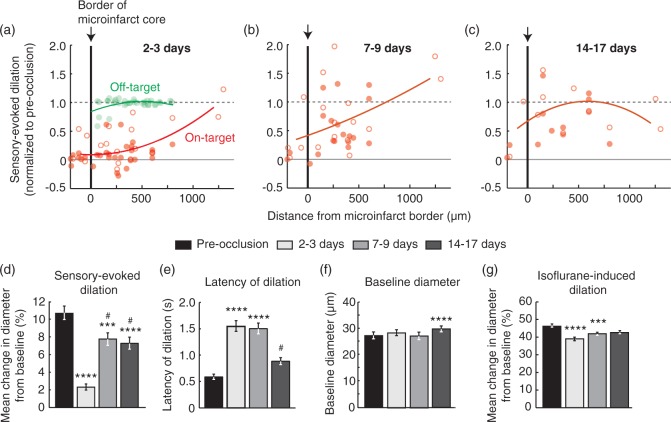
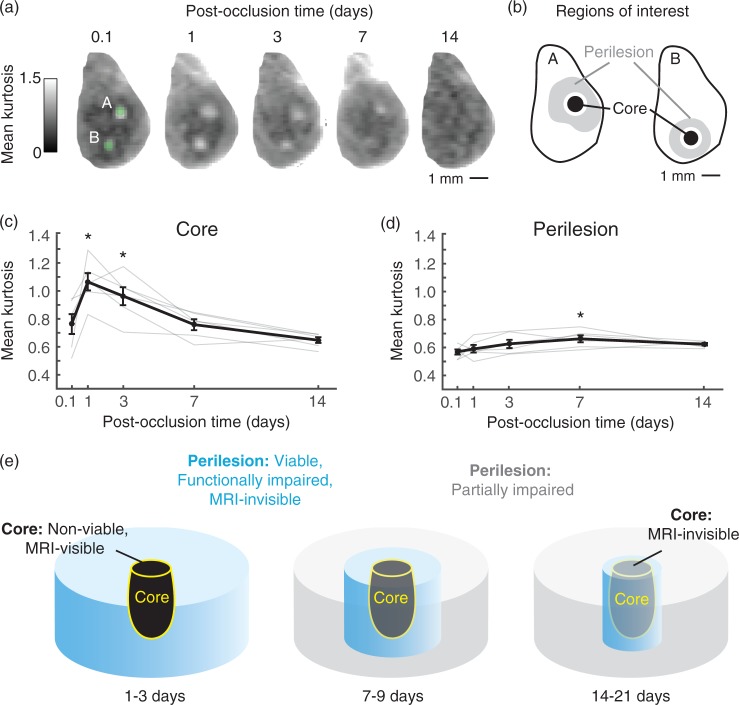
Clinical studies have revealed a strong link between increased burden of cerebral microinfarcts and risk for cognitive impairment. Since the sum of tissue damage incurred by microinfarcts is a miniscule percentage of total brain volume, we hypothesized that microinfarcts disrupt brain function beyond the injury site visible to histological or radiological examination. We tested this idea using a mouse model of microinfarcts, where single penetrating vessels that supply mouse cortex were occluded by targeted photothrombosis. We found that in vivo structural and diffusion MRI reliably reported the acute microinfarct core, based on spatial co-registrations with post-mortem stains of neuronal viability. Consistent with our hypothesis, c-Fos assays for neuronal activity and in vivo imaging of single vessel hemodynamics both reported functional deficits in viable peri-lesional tissues beyond the microinfarct core. We estimated that the volume of tissue with functional deficit in cortex was at least 12-fold greater than the volume of the microinfarct core. Impaired hemodynamic responses in peri-lesional tissues persisted at least 14 days, and were attributed to lasting deficits in neuronal circuitry or neurovascular coupling. These data show how individually miniscule microinfarcts could contribute to broader brain dysfunction during vascular cognitive impairment and dementia.
Keywords: Microinfarcts; microcirculation; neurovascular coupling; two-photon microscopy; vascular cognitive impairment.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
