

Results of a randomized controlled trial analyzing telemedically supported case management in the first year after living donor kidney transplantation - a budget impact analysis from the healthcare perspective
- PMID: 28092012
- PMCID: PMC5236052
- DOI: 10.1186/s13561-016-0141-3
Results of a randomized controlled trial analyzing telemedically supported case management in the first year after living donor kidney transplantation - a budget impact analysis from the healthcare perspective
Abstract
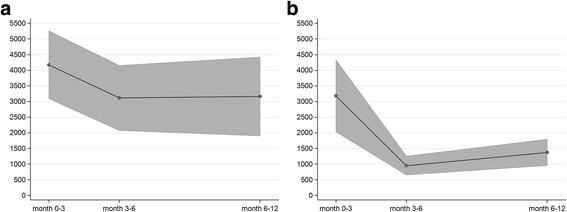
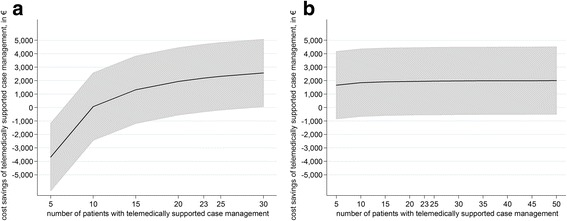
ᅟ: We analyze one-year costs and savings of a telemedically supported case management program after kidney transplantation from the perspective of the German Healthcare System. Recipients of living donor kidney transplantation (N = 46) were randomly allocated to either (1) standard aftercare or (2) standard aftercare plus additional telemedically supported case management. A range of cost figures of each patient's medical service utilization were calculated at month 3, 6 and 12 and analyzed using two-part regression models. In comparison to standard aftercare, patients receiving telemedically supported case management are associated with substantial lower costs related to unscheduled hospitalizations (mean difference: €3,417.46 per patient for the entire one-year period, p = 0.003). Taking all cost figures into account, patients receiving standard aftercare are associated, on average, with one-year medical service utilization costs of €10,449.28, while patients receiving telemedically supported case management are associated with €5,504.21 of costs (mean difference: € 4,945.07 per patient, p < 0.001). With estimated expenditures of €3,001.5 for telemedically supported case management of a single patient, we determined a mean difference of €1,943.57, but this result is not statistically significant (p = 0.128). Sensitivity analyses show that the program becomes cost-neutral at around ten participating patients, and was beneficial starting at 15 patients. Routine implementation of telemedically supported case management in German medium and high-volume transplant centers would result in annual cost savings of €791,033 for the German healthcare system. Patients with telemedically supported case management showed a lower utilization of medical services as well as better medical outcomes. Therefore, such programs should be implemented in medium and high-volume transplant centers.
Trial registration: DRKS00007634 ( http://www.drks.de/DRKS00007634 ).
Keywords: Cost-benefit; Cost-of-illness; Telemedicine.
Figures
References
-
- Sellares J, De Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF. Understanding the Causes of Kidney Transplant Failure: The Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am J Transplant. 2012;12:388–399. doi: 10.1111/j.1600-6143.2011.03840.x. - DOI - PubMed
-
- Gremigni P, Bacchi F, Turrini C, Cappelli G, Albertazzi A, Bitti PER. Psychological factors associated with medication adherence following renal transplantation. Clin Transpl. 2007;21:710–715. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
