

Machine Learning of Three-dimensional Right Ventricular Motion Enables Outcome Prediction in Pulmonary Hypertension: A Cardiac MR Imaging Study
- PMID: 28092203
- PMCID: PMC5398374
- DOI: 10.1148/radiol.2016161315
Machine Learning of Three-dimensional Right Ventricular Motion Enables Outcome Prediction in Pulmonary Hypertension: A Cardiac MR Imaging Study
Abstract
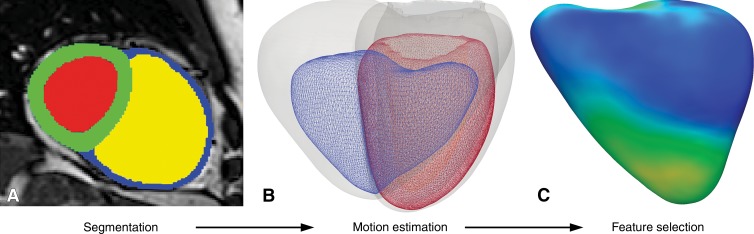
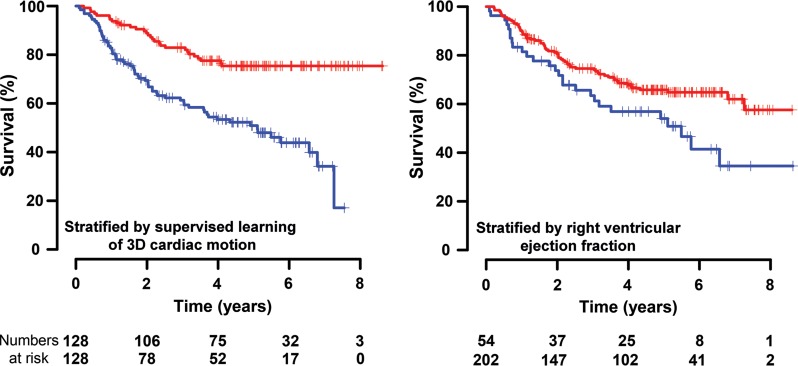
Purpose To determine if patient survival and mechanisms of right ventricular failure in pulmonary hypertension could be predicted by using supervised machine learning of three-dimensional patterns of systolic cardiac motion. Materials and Methods The study was approved by a research ethics committee, and participants gave written informed consent. Two hundred fifty-six patients (143 women; mean age ± standard deviation, 63 years ± 17) with newly diagnosed pulmonary hypertension underwent cardiac magnetic resonance (MR) imaging, right-sided heart catheterization, and 6-minute walk testing with a median follow-up of 4.0 years. Semiautomated segmentation of short-axis cine images was used to create a three-dimensional model of right ventricular motion. Supervised principal components analysis was used to identify patterns of systolic motion that were most strongly predictive of survival. Survival prediction was assessed by using difference in median survival time and area under the curve with time-dependent receiver operating characteristic analysis for 1-year survival. Results At the end of follow-up, 36% of patients (93 of 256) died, and one underwent lung transplantation. Poor outcome was predicted by a loss of effective contraction in the septum and free wall, coupled with reduced basal longitudinal motion. When added to conventional imaging and hemodynamic, functional, and clinical markers, three-dimensional cardiac motion improved survival prediction (area under the receiver operating characteristic curve, 0.73 vs 0.60, respectively; P < .001) and provided greater differentiation according to difference in median survival time between high- and low-risk groups (13.8 vs 10.7 years, respectively; P < .001). Conclusion A machine-learning survival model that uses three-dimensional cardiac motion predicts outcome independent of conventional risk factors in patients with newly diagnosed pulmonary hypertension. Online supplemental material is available for this article.
Figures





References
-
- Galiè N, Humbert M, Vachiery JL, et al. . 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J 2015;46(4):903–975. - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, et al. . Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 2010;122(2):164–172. - PubMed
-
- Vonk-Noordegraaf A, Haddad F, Chin KM, et al. . Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol 2013;62(25 Suppl):D22–D33. - PubMed
-
- van de Veerdonk MC, Kind T, Marcus JT, et al. . Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J Am Coll Cardiol 2011;58(24):2511–2519. - PubMed
-
- Naeije R, Ghio S. More on the right ventricle in pulmonary hypertension. Eur Respir J 2015;45(1):33–35. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
