

Is Enhanced Recovery the New Standard of Care in Microsurgical Breast Reconstruction?
- PMID: 28092334
- PMCID: PMC5640259
- DOI: 10.1097/PRS.0000000000003235
Is Enhanced Recovery the New Standard of Care in Microsurgical Breast Reconstruction?
Abstract
Background: At present, there are limited data available regarding the use and feasibility of enhanced recovery pathways for patients undergoing microsurgical breast reconstruction. The authors sought to assess patient outcomes before and after the introduction of an enhanced recovery pathway that was adopted at a single cancer center.
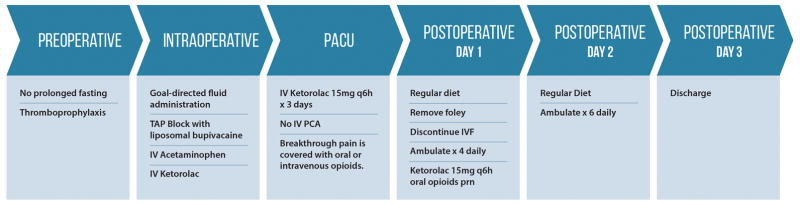
Methods: A multidisciplinary enhanced recovery pathway was developed for patients undergoing deep inferior epigastric perforator or free transverse rectus abdominis myocutaneous flap breast reconstruction. Core elements of the enhanced recovery pathway included substituting intravenous patient-controlled analgesia with ketorolac and transversus abdominis plane blocks using liposomal bupivacaine, as well as intraoperative goal-directed fluid management. Patients who underwent surgery between April and August of 2015 using the enhanced recovery pathway were compared with a historical control cohort. The primary endpoints were hospital length of stay and total postoperative opioid consumption.
Results: In total, 91 consecutive patients were analyzed (enhanced recovery pathway, n = 42; pre-enhanced recovery pathway, n = 49). Mean hospital length of stay was significantly shorter in the enhanced recovery pathway group than in the pre-enhanced recovery pathway group (4.0 days versus 5.0 days; p < 0.0001). Total postoperative morphine equivalent consumption was also lower in the enhanced recovery pathway group (46.0 mg versus 70.5 mg; p = 0.003). There was no difference in the incidence of 30-day complications between the groups (p = 0.6).
Conclusion: The adoption of an enhanced recovery pathway for deep inferior epigastric perforator and transverse rectus abdominis myocutaneous flap reconstruction by multiple surgeons significantly decreased opioid consumption and reduced length of stay by 1 day.
Clinical question/level of evidence: Therapeutic, III.
Conflict of interest statement
Figures
References
-
- Nelson JA, Fischer JP, Pasick C, et al. Chronic pain following abdominal free flap breast reconstruction: a prospective pilot analysis. Ann Plast Surg. 2013;71:278–282. - PubMed
-
- Gartner R, Kroman N, Callesen T, Kehlet H. Multimodal prevention of pain, nausea and vomiting after breast cancer surgery. Minerva Anestesiol. 2010;76:805–813. - PubMed
-
- Batdorf NJ, Lemaine V, Lovely JK, et al. Enhanced recovery after surgery in microvascular breast reconstruction. J Plast Reconstr Aesthet Surg. 2015;68:395–402. - PubMed
-
- Hainsworth AJ, Lobo CR, Williams P, et al. ‘23 h Model’ for breast surgery: an early experience. Breast. 2013;22:898–901. - PubMed
-
- Bonde C, Khorasani H, Eriksen K, Wolthers M, Kehlet H, Elberg J. Introducing the fast track surgery principles can reduce length of stay after autologous breast reconstruction using free flaps: A case control study. J Plast Surg Hand Surg. 2015;49:367–371. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
