

Loss of μ opioid receptor signaling in nociceptors, but not microglia, abrogates morphine tolerance without disrupting analgesia
- PMID: 28092666
- PMCID: PMC5296291
- DOI: 10.1038/nm.4262
Loss of μ opioid receptor signaling in nociceptors, but not microglia, abrogates morphine tolerance without disrupting analgesia
Abstract
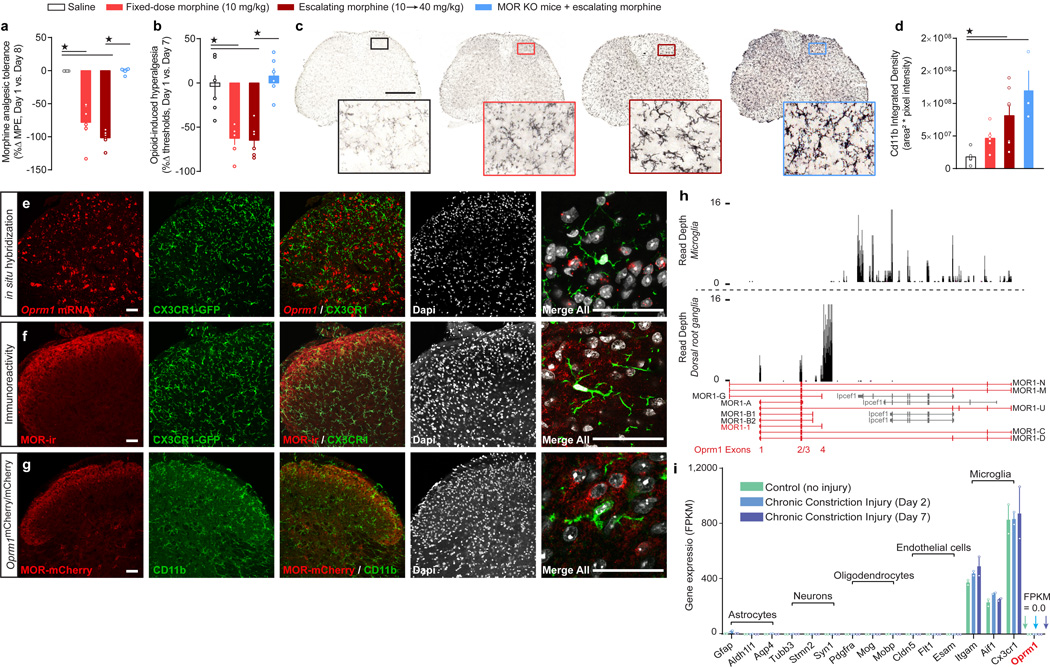
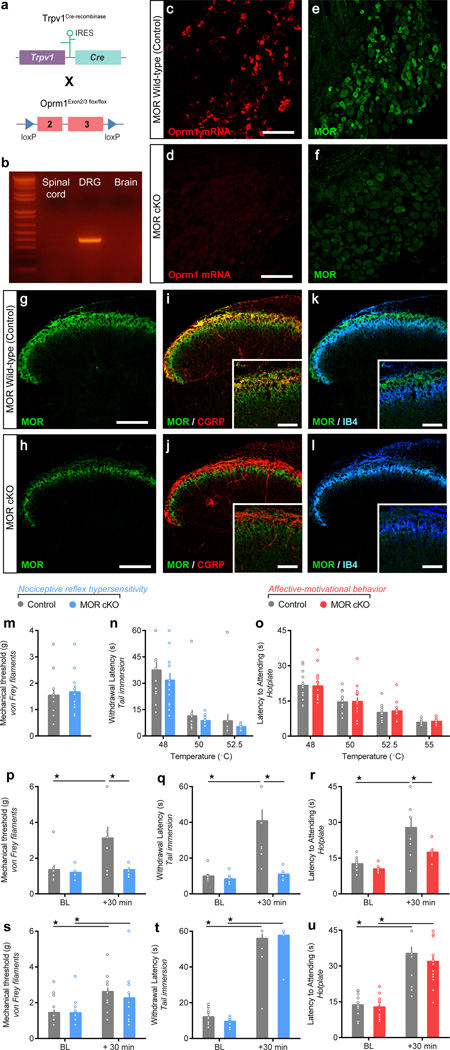
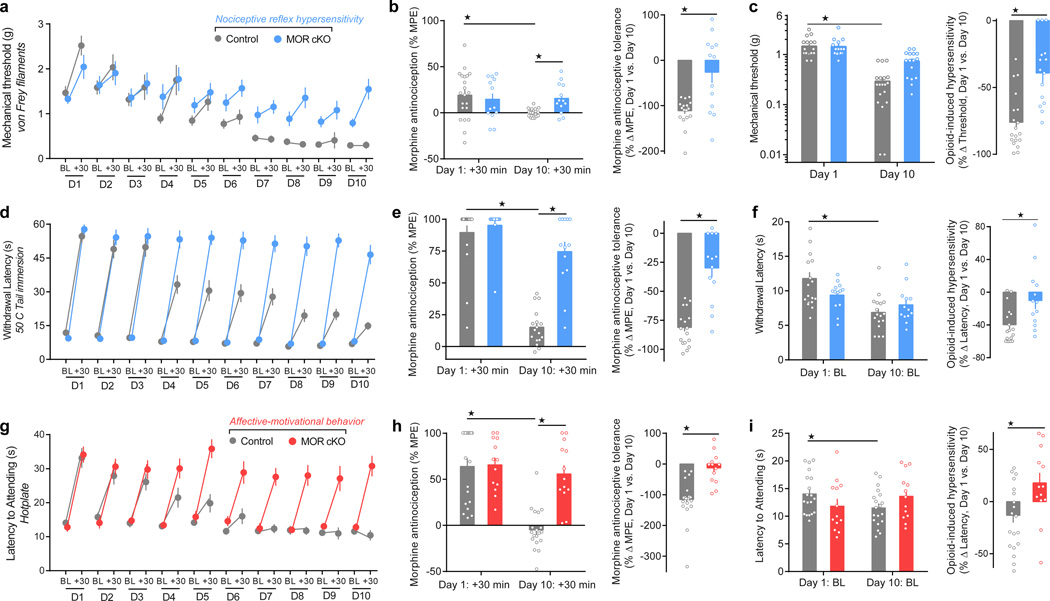
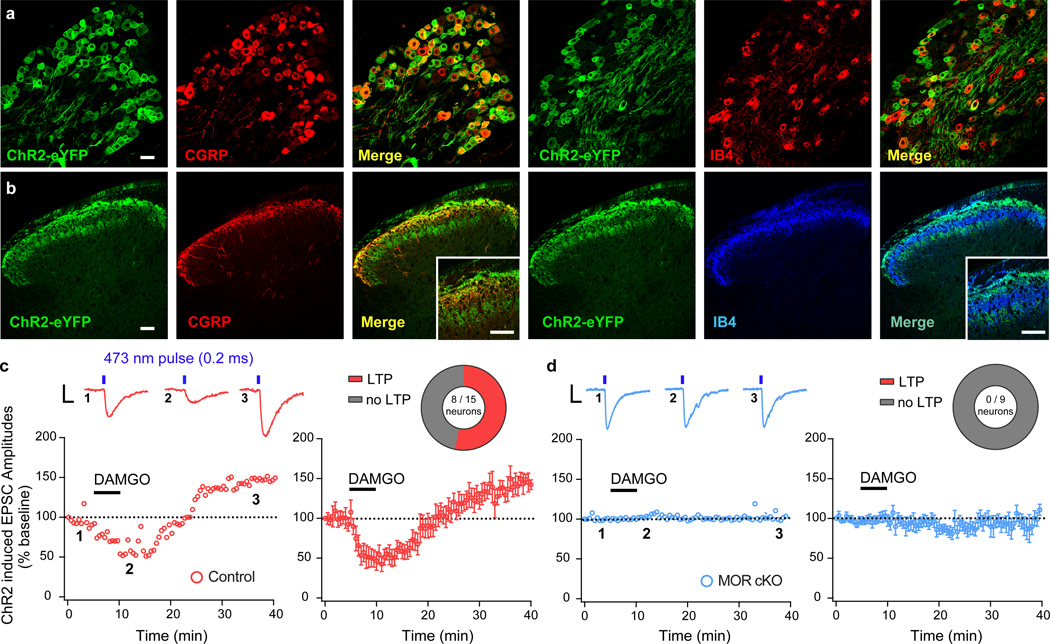
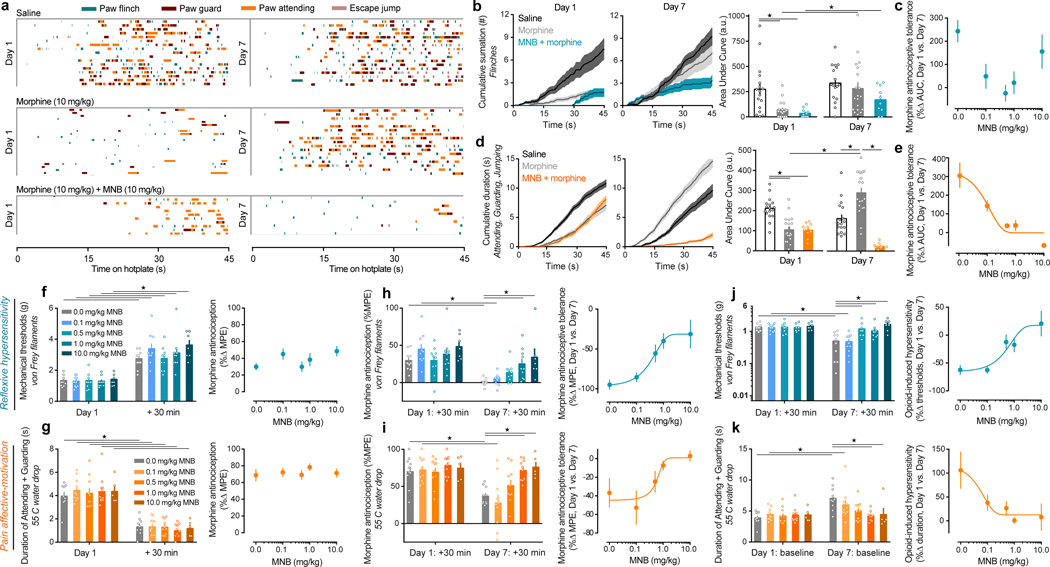
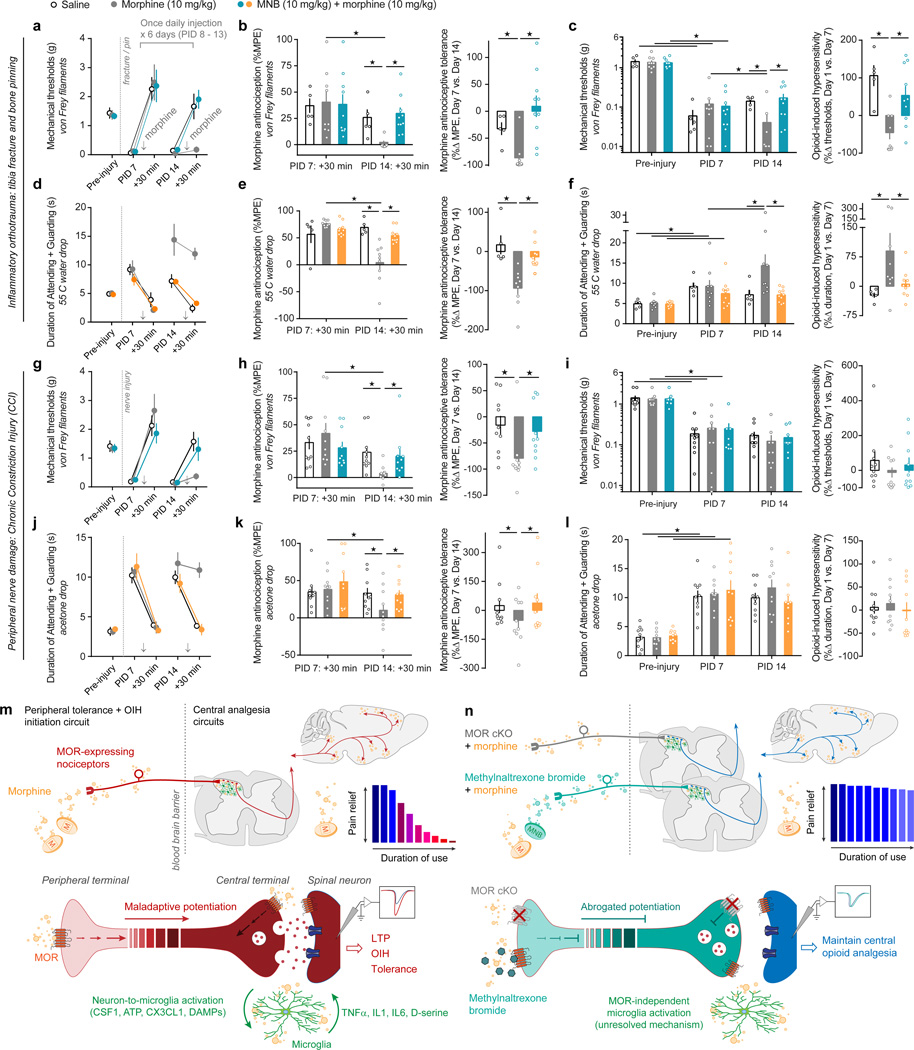
Opioid pain medications have detrimental side effects including analgesic tolerance and opioid-induced hyperalgesia (OIH). Tolerance and OIH counteract opioid analgesia and drive dose escalation. The cell types and receptors on which opioids act to initiate these maladaptive processes remain disputed, which has prevented the development of therapies to maximize and sustain opioid analgesic efficacy. We found that μ opioid receptors (MORs) expressed by primary afferent nociceptors initiate tolerance and OIH development. RNA sequencing and histological analysis revealed that MORs are expressed by nociceptors, but not by spinal microglia. Deletion of MORs specifically in nociceptors eliminated morphine tolerance, OIH and pronociceptive synaptic long-term potentiation without altering antinociception. Furthermore, we found that co-administration of methylnaltrexone bromide, a peripherally restricted MOR antagonist, was sufficient to abrogate morphine tolerance and OIH without diminishing antinociception in perioperative and chronic pain models. Collectively, our data support the idea that opioid agonists can be combined with peripheral MOR antagonists to limit analgesic tolerance and OIH.
Figures
Comment in
-
New connections: Getting the good without the bad, opiate edition.Sci Signal. 2017 Mar 21;10(471):eaan2516. doi: 10.1126/scisignal.aan2516. Sci Signal. 2017. PMID: 28325819
References
-
- Carroll IR, Angst MS, Clark JD. Management of perioperative pain in patients chronically consuming opioids. Reg. Anesth. Pain Med. 2004;29:576–591. - PubMed
-
- Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids in chronic non-cancer pain: Systematic review of efficacy and safety. Pain. 2004;112:372–380. - PubMed
-
- A. Pizzo P, M. Clark N, Carter Pokras O. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Institute of Medicin. 2011
-
- Volkow N, McLellan T. Opioid Abuse in Chronic Pain — Misconceptions and Mitigation Strategies. N. Engl. J. Med. 2016;374 - PubMed
-
- Chu LF, Angst MS, Clark D. Opioid-induced hyperalgesia in humans: molecular mechanisms and clinical considerations. Clin. J. Pain. 2008;24:479–496. - PubMed
METHODS-ONLY REFERENCES
-
- Sorge RE, et al. Olfactory exposure to males, including men, causes stress and related analgesia in rodents. Nat. Methods. 2014;11:629–632. - PubMed
-
- Mogil JS. Animal models of pain: progress and challenges. Nat. Rev. Neurosci. 2009;10:283–294. - PubMed
-
- Woolf CJ. Long term alterations in the excitability of the flexion reflex produced by peripheral tissue injury in the chronic decerebrate rat. Pain. 1984;18:325–343. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
