

Beyond Bernoulli: Improving the Accuracy and Precision of Noninvasive Estimation of Peak Pressure Drops
- PMID: 28093412
- PMCID: PMC5265685
- DOI: 10.1161/CIRCIMAGING.116.005207
Beyond Bernoulli: Improving the Accuracy and Precision of Noninvasive Estimation of Peak Pressure Drops
Abstract
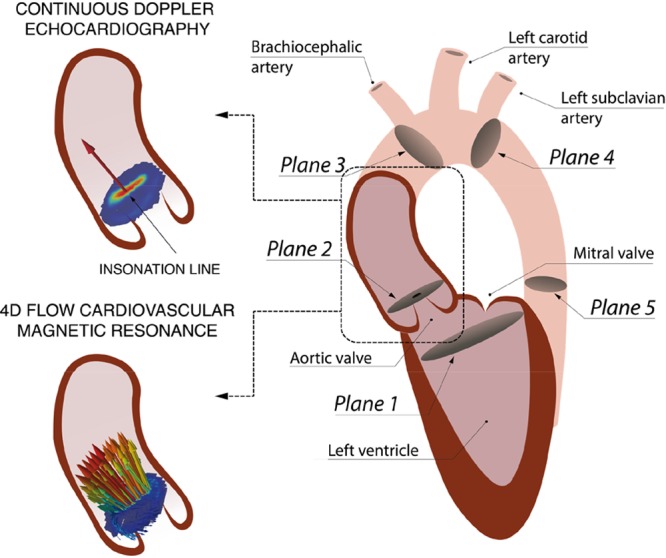
Background: Transvalvular peak pressure drops are routinely assessed noninvasively by echocardiography using the Bernoulli principle. However, the Bernoulli principle relies on several approximations that may not be appropriate, including that the majority of the pressure drop is because of the spatial acceleration of the blood flow, and the ejection jet is a single streamline (single peak velocity value).
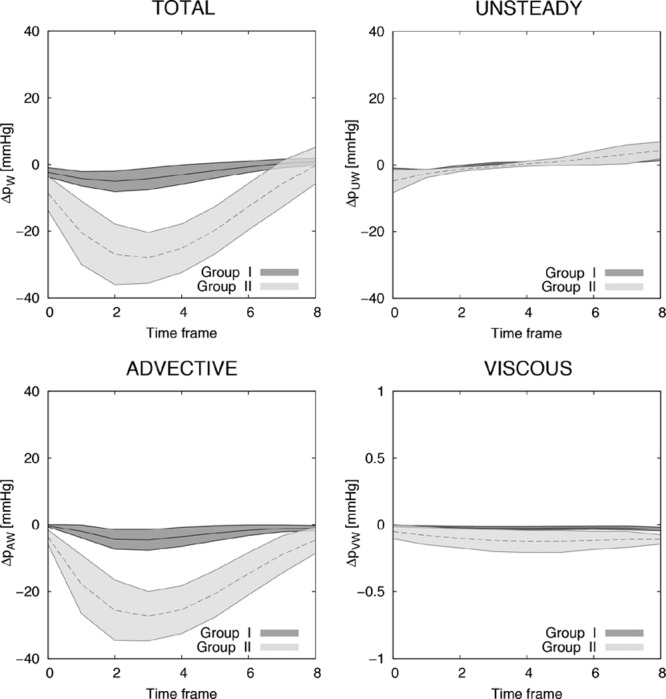
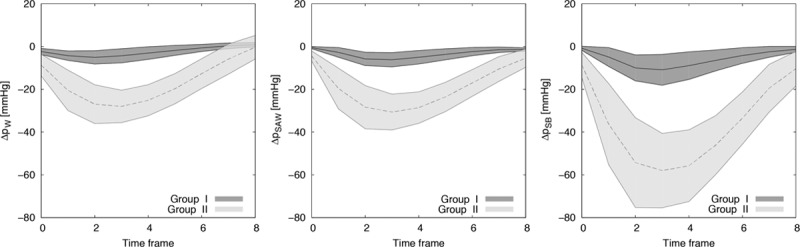
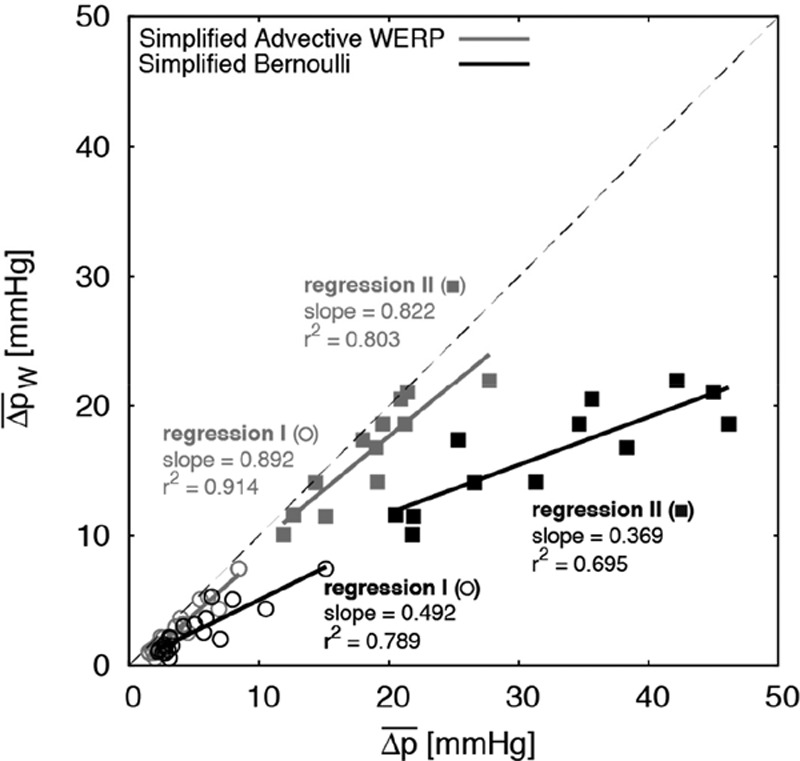
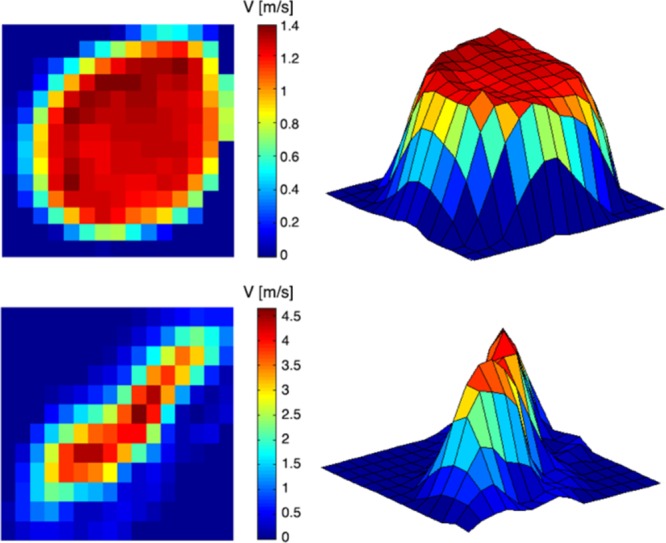
Methods and results: We assessed the accuracy of the Bernoulli principle to estimate the peak pressure drop at the aortic valve using 3-dimensional cardiovascular magnetic resonance flow data in 32 subjects. Reference pressure drops were computed from the flow field, accounting for the principles of physics (ie, the Navier-Stokes equations). Analysis of the pressure components confirmed that the spatial acceleration of the blood jet through the valve is most significant (accounting for 99% of the total drop in stenotic subjects). However, the Bernoulli formulation demonstrated a consistent overestimation of the transvalvular pressure (average of 54%, range 5%-136%) resulting from the use of a single peak velocity value, which neglects the velocity distribution across the aortic valve plane. This assumption was a source of uncontrolled variability.
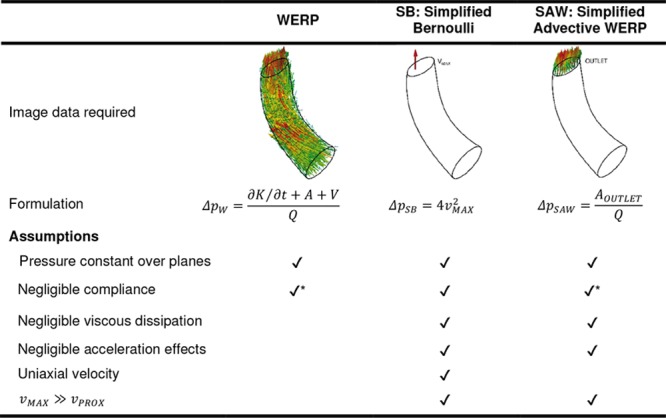
Conclusions: The application of the Bernoulli formulation results in a clinically significant overestimation of peak pressure drops because of approximation of blood flow as a single streamline. A corrected formulation that accounts for the cross-sectional profile of the blood flow is proposed and adapted to both cardiovascular magnetic resonance and echocardiographic data.
Keywords: Bernoulli principle; biomarker; blood pressure; hemodynamics; stenosis; valve.
© 2017 The Authors.
Figures
Comment in
-
Noninvasive Estimation of the Severity of Aortic Stenosis: Going Beyond Bernoulli.Circ Cardiovasc Imaging. 2017 Jan;10(1):e005967. doi: 10.1161/CIRCIMAGING.116.005967. Circ Cardiovasc Imaging. 2017. PMID: 28093416 No abstract available.
References
-
- Cioffi G, Faggiano P, Vizzardi E, Tarantini L, Cramariuc D, Gerdts E, de Simone G. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart. 2011;97:301–307. doi: 10.1136/hrt.2010.192997. - PubMed
-
- Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, Iung B, Otto CM, Pellikka PA, Quiñones M American Society of Echocardiography; European Association of Echocardiography. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009;22:1–23; quiz 101. doi: 10.1016/j.echo.2008.11.029. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM, 3rd, Thomas JD American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:2440–2492. doi: 10.1161/CIR.0000000000000029. - PubMed
-
- Baumgartner H, Stefenelli T, Niederberger J, Schima H, Maurer G. “Overestimation” of catheter gradients by Doppler ultrasound in patients with aortic stenosis: a predictable manifestation of pressure recovery. J Am Coll Cardiol. 1999;33:1655–1661. - PubMed
-
- Garcia D, Dumesnil JG, Durand LG, Kadem L, Pibarot P. Discrepancies between catheter and Doppler estimates of valve effective orifice area can be predicted from the pressure recovery phenomenon: practical implications with regard to quantification of aortic stenosis severity. J Am Coll Cardiol. 2003;41:435–442. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
