

Tumor-Infiltrating Merkel Cell Polyomavirus-Specific T Cells Are Diverse and Associated with Improved Patient Survival
- PMID: 28093446
- PMCID: PMC5421625
- DOI: 10.1158/2326-6066.CIR-16-0210
Tumor-Infiltrating Merkel Cell Polyomavirus-Specific T Cells Are Diverse and Associated with Improved Patient Survival
Abstract
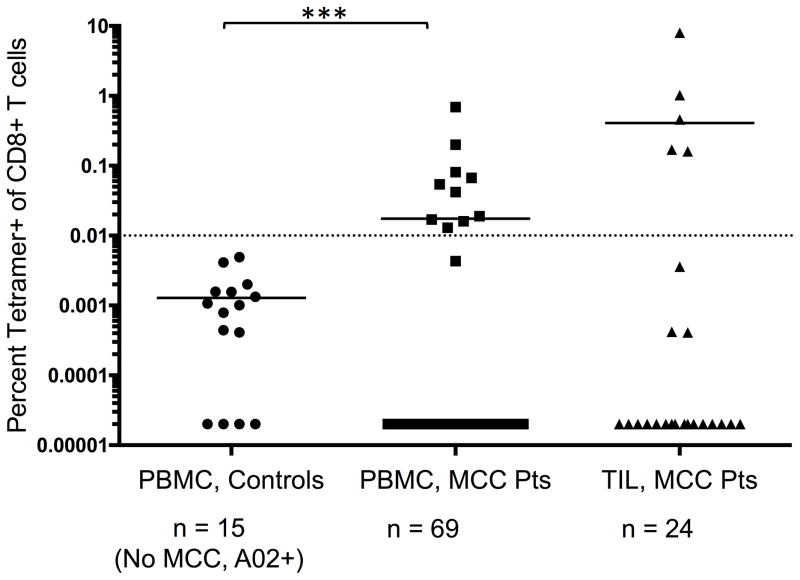
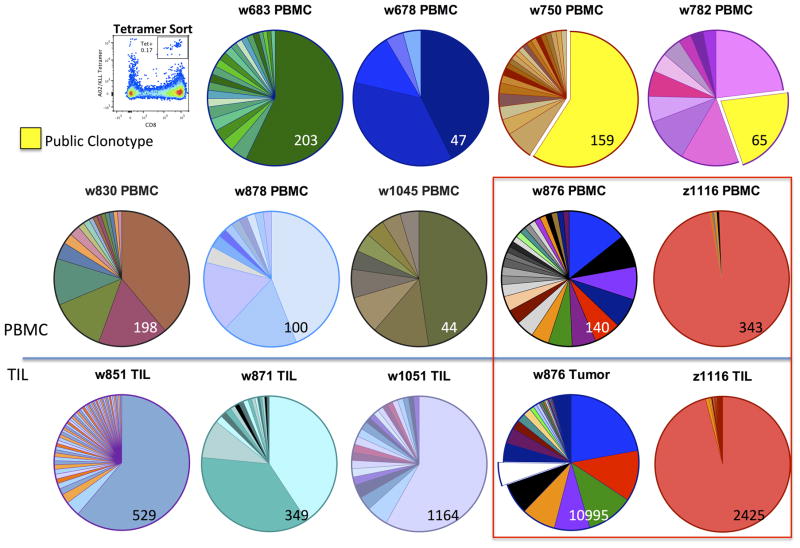
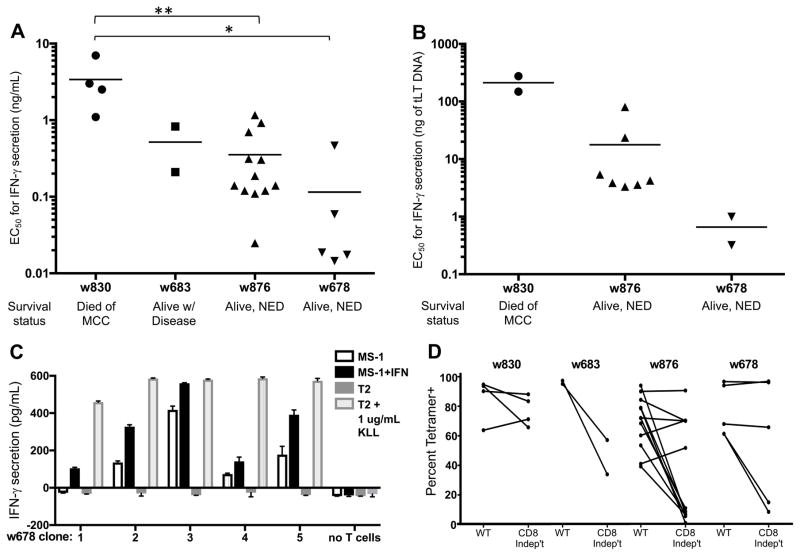
Tumor-infiltrating CD8+ T cells are associated with improved survival of patients with Merkel cell carcinoma (MCC), an aggressive skin cancer causally linked to Merkel cell polyomavirus (MCPyV). However, CD8+ T-cell infiltration is robust in only 4% to 18% of MCC tumors. We characterized the T-cell receptor (TCR) repertoire restricted to one prominent epitope of MCPyV (KLLEIAPNC, "KLL") and assessed whether TCR diversity, tumor infiltration, or T-cell avidity correlated with clinical outcome. HLA-A*02:01/KLL tetramer+ CD8+ T cells from MCC patient peripheral blood mononuclear cells (PBMC) and tumor-infiltrating lymphocytes (TIL) were isolated via flow cytometry. TCRβ (TRB) sequencing was performed on tetramer+ cells from PBMCs or TILs (n = 14) and matched tumors (n = 12). Functional avidity of T-cell clones was determined by IFNγ production. We identified KLL tetramer+ T cells in 14% of PBMC and 21% of TIL from MCC patients. TRB repertoires were strikingly diverse (397 unique TRBs were identified from 12 patients) and mostly private (only one TCRb clonotype shared between two patients). An increased fraction of KLL-specific TIL (>1.9%) was associated with significantly increased MCC-specific survival P = 0.0009). T-cell cloning from four patients identified 42 distinct KLL-specific TCRa/b pairs. T-cell clones from patients with improved MCC-specific outcomes were more avid (P < 0.05) and recognized an HLA-appropriate MCC cell line. T cells specific for a single MCPyV epitope display marked TCR diversity within and between patients. Intratumoral infiltration by MCPyV-specific T cells was associated with significantly improved MCC-specific survival, suggesting that augmenting the number or avidity of virus-specific T cells may have therapeutic benefit. Cancer Immunol Res; 5(2); 137-47. ©2017 AACR.
©2017 American Association for Cancer Research.
Conflict of interest statement
PN serves as a paid consultant for EMD Serono.
Figures


References
-
- Allen PJ. Merkel Cell Carcinoma: Prognosis and Treatment of Patients From a Single Institution. J Clin Oncol. 2005;23:2300–2309. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
