

Rapid adaptation drives invasion of airway donor microbiota by Pseudomonas after lung transplantation
- PMID: 28094327
- PMCID: PMC5240337
- DOI: 10.1038/srep40309
Rapid adaptation drives invasion of airway donor microbiota by Pseudomonas after lung transplantation
Abstract
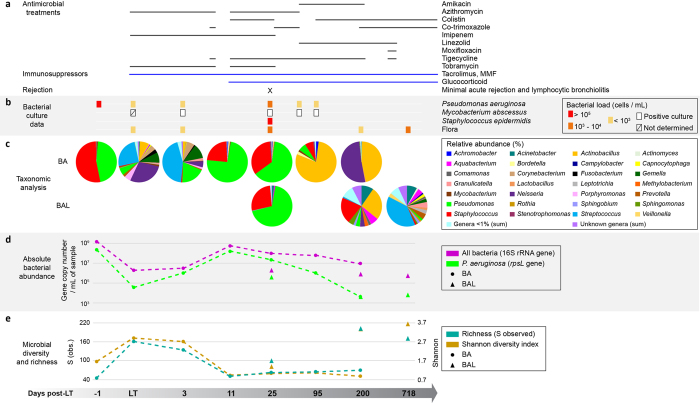
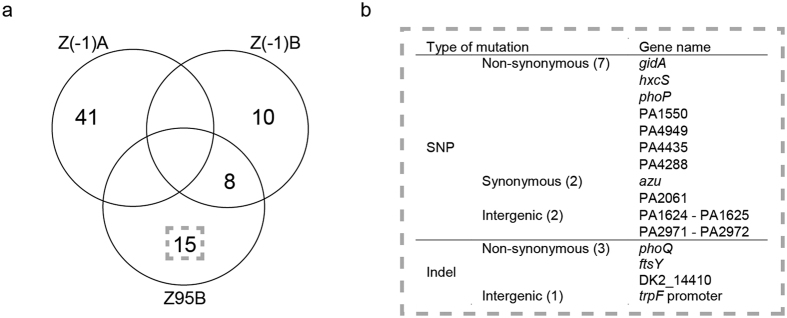
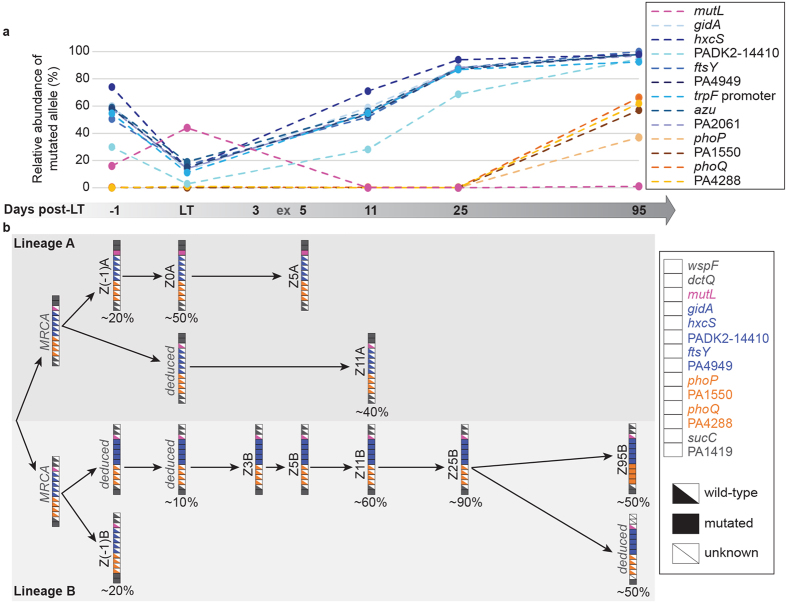
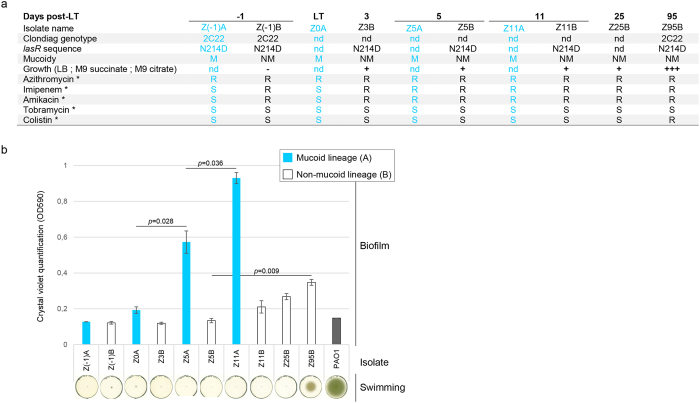
In cystic fibrosis (CF) patients, chronic airway infection by Pseudomonas leads to progressive lung destruction ultimately requiring lung transplantation (LT). Following LT, CF-adapted Pseudomonas strains, potentially originating from the sinuses, may seed the allograft leading to infections and reduced allograft survival. We investigated whether CF-adapted Pseudomonas populations invade the donor microbiota and adapt to the non-CF allograft. We collected sequential Pseudomonas isolates and airway samples from a CF-lung transplant recipient during two years, and followed the dynamics of the microbiota and Pseudomonas populations. We show that Pseudomonas invaded the host microbiota within three days post-LT, in association with a reduction in richness and diversity. A dominant mucoid and hypermutator mutL lineage was replaced after 11 days by non-mucoid strains. Despite antibiotic therapy, Pseudomonas dominated the allograft microbiota until day 95. We observed positive selection of pre-LT variants and the appearance of novel mutations. Phenotypic adaptation resulted in increased biofilm formation and swimming motility capacities. Pseudomonas was replaced after 95 days by a microbiota dominated by Actinobacillus. In conclusion, mucoid Pseudomonas adapted to the CF-lung remained able to invade the allograft. Selection of both pre-existing non-mucoid subpopulations and of novel phenotypic traits suggests rapid adaptation of Pseudomonas to the non-CF allograft.
Figures
References
-
- Christie J. D. et al. The Registry of the International Society for Heart and Lung Transplantation: Twenty-sixth Official Adult Lung and Heart-Lung Transplantation Report-2009. The Journal of heart and lung transplantation: the official publication of the International Society for Heart Transplantation 28, 1031–1049, doi: 10.1016/j.healun.2009.08.004 (2009). - DOI - PubMed
-
- Foundation C. F. Cystic Fibrosis Foundation patient registry 2010 annual data report. (2011).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
