

Medical Oncologists' Experiences in Using Genomic Testing for Lung and Colorectal Cancer Care
- PMID: 28095174
- PMCID: PMC5456256
- DOI: 10.1200/JOP.2016.016659
Medical Oncologists' Experiences in Using Genomic Testing for Lung and Colorectal Cancer Care
Abstract
Purpose: Genomic testing improves outcomes for many at-risk individuals and patients with cancer; however, little is known about how genomic testing for non-small-cell lung cancer (NSCLC) and colorectal cancer (CRC) is used in clinical practice.
Patients and methods: In 2012 to 2013, we surveyed medical oncologists who care for patients in diverse practice and health care settings across the United States about their use of guideline- and non-guideline-endorsed genetic tests. Multivariable regression models identified factors that are associated with greater test use.
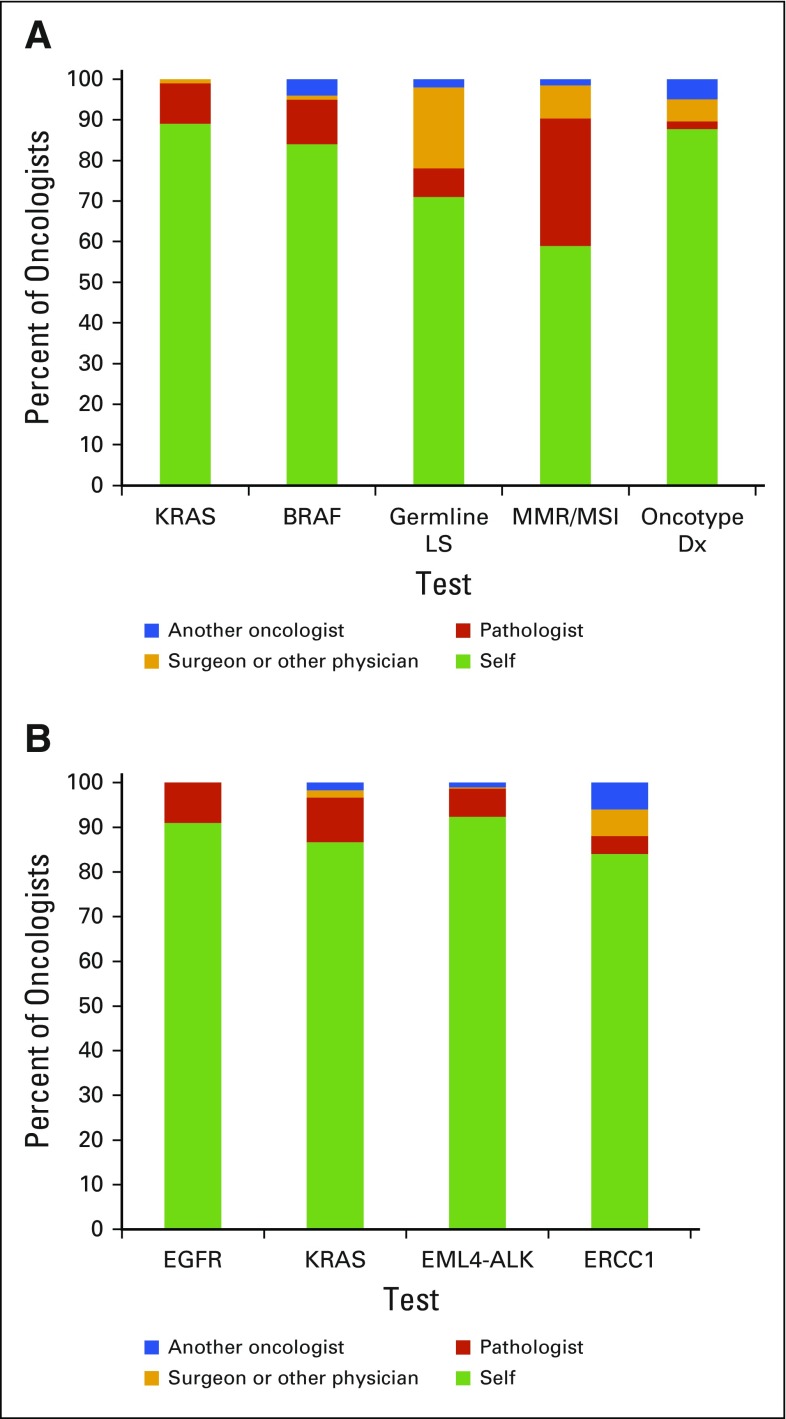
Results: Of oncologists, 337 completed the survey (participation rate, 53%). Oncologists reported higher use of guideline-endorsed tests (eg, KRAS for CRC; EGFR for NSCLC) than non-guideline-endorsed tests (eg, Onco typeDX Colon; ERCC1 for NSCLC). Many oncologists reported having no patients with CRC who had mismatch repair and/or microsatellite instability (24%) or germline Lynch syndrome (32%) testing, and no patients with NSCLC who had ALK testing (11%). Of oncologists, 32% reported that five or fewer patients had KRAS and EGFR testing for CRC and NSCLC, respectively. Oncologists, rather than pathologists or surgeons, ordered the vast majority of tests. In multivariable analyses, fewer patients in nonprofit integrated health care delivery systems underwent testing than did patients in hospital or office-based single-specialty group settings (all P < .05). High patient volume and patient requests (CRC only) were also associated with higher test use (all P < .05).
Conclusion: Genomic test use for CRC and NSCLC varies by test and practice characteristics. Research in specific clinical contexts is needed to determine whether the observed variation reflects appropriate or inappropriate care. One potential way to reduce unwanted variation would be to offer widespread reflexive testing by pathology for guideline-endorsed predictive somatic tests.
Figures
References
-
- National Comprehensive Cancer Network: NCCN clinical practice guidelines in oncology–Genetic/familial high-risk assessment: Breast and ovarian. https://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf - PubMed
-
- National Comprehensive Cancer Network NCCN clinical practice guidelines in oncology–Non-small cell lung cancer. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf
-
- National Comprehensive Cancer Network NCCN clinical practice guidelines in oncology–Colon cancer. https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf - PubMed
-
- Pujol P, Lyonnet DS, Frebourg T, et al. Lack of referral for genetic counseling and testing in BRCA1/2 and Lynch syndromes: A nationwide study based on 240,134 consultations and 134,652 genetic tests. Breast Cancer Res Treat. 2013;141:135–144. - PubMed
-
- Wideroff L, Freedman AN, Olson L, et al. Physician use of genetic testing for cancer susceptibility: Results of a national survey. Cancer Epidemiol Biomarkers Prev. 2003;12:295–303. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
