

Impact of Increasing Age on Cause-Specific Mortality and Morbidity in Patients With Stage I Non-Small-Cell Lung Cancer: A Competing Risks Analysis
- PMID: 28095268
- PMCID: PMC5456376
- DOI: 10.1200/JCO.2016.69.0834
Impact of Increasing Age on Cause-Specific Mortality and Morbidity in Patients With Stage I Non-Small-Cell Lung Cancer: A Competing Risks Analysis
Abstract
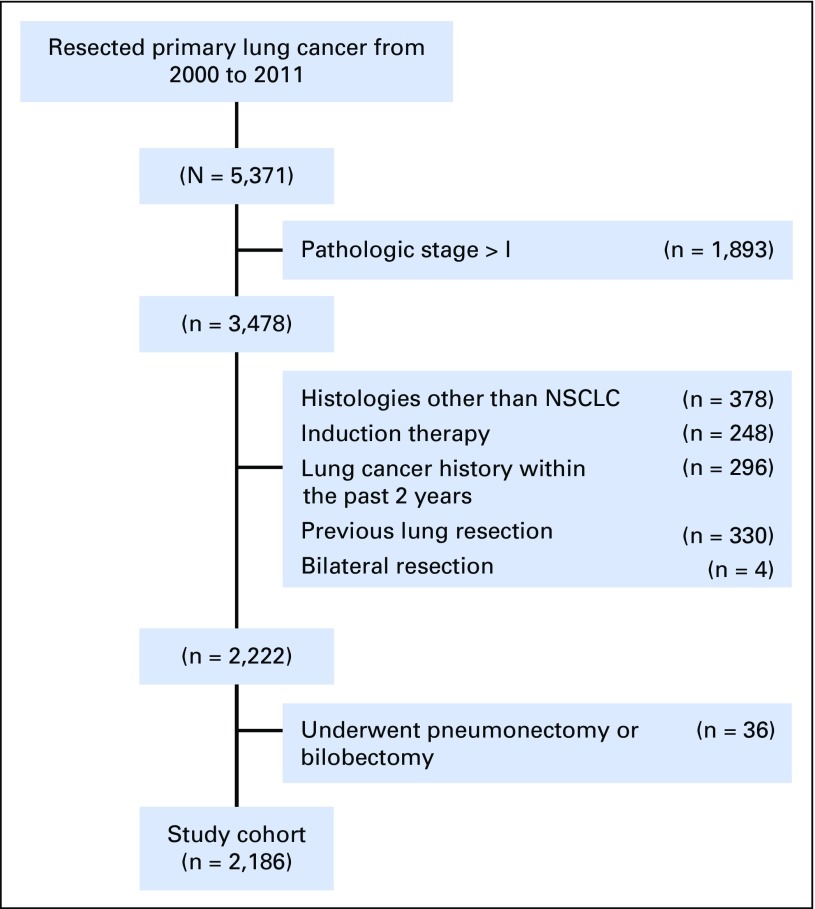
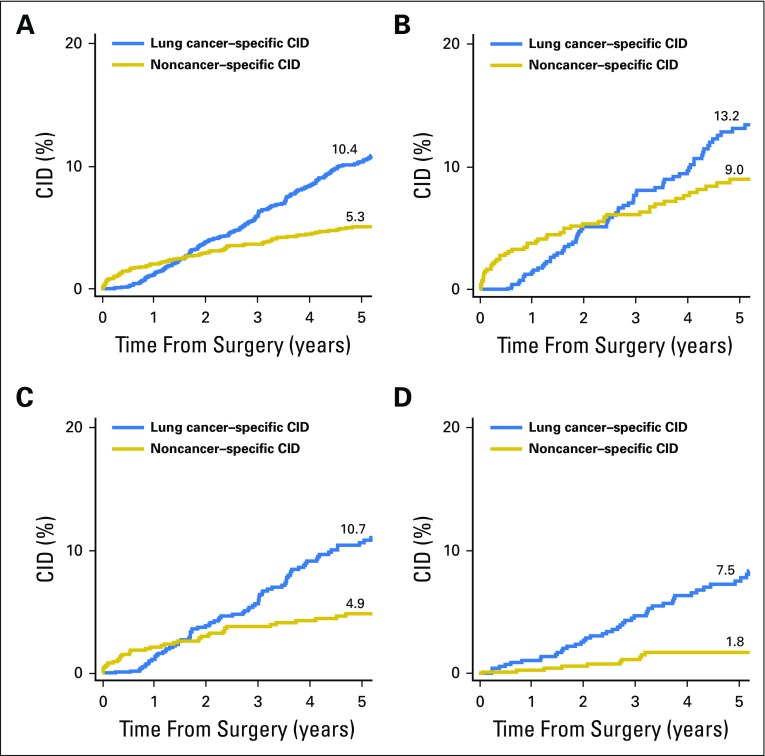
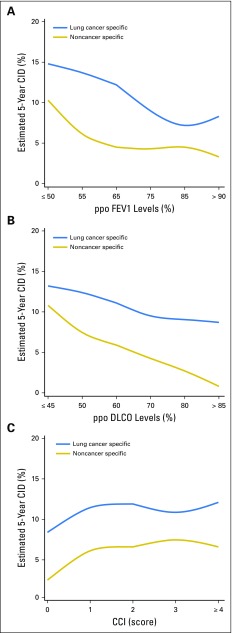
Purpose To perform competing risks analysis and determine short- and long-term cancer- and noncancer-specific mortality and morbidity in patients who had undergone resection for stage I non-small-cell lung cancer (NSCLC). Patients and Methods Of 5,371 consecutive patients who had undergone curative-intent resection of primary lung cancer at our institution (2000 to 2011), 2,186 with pathologic stage I NSCLC were included in the analysis. All preoperative clinical variables known to affect outcomes were included in the analysis, specifically, Charlson comorbidity index, predicted postoperative (ppo) diffusing capacity of the lung for carbon monoxide, and ppo forced expiratory volume in 1 second. Cause-specific mortality analysis was performed with competing risks analysis. Results Of 2,186 patients, 1,532 (70.1%) were ≥ 65 years of age, including 638 (29.2%) ≥ 75 years of age. In patients < 65, 65 to 74, and ≥ 75 years of age, 5-year lung cancer-specific cumulative incidence of death (CID) was 7.5%, 10.7%, and 13.2%, respectively (overall, 10.4%); noncancer-specific CID was 1.8%, 4.9%, and 9.0%, respectively (overall, 5.3%). In patients ≥ 65 years of age, for up to 2.5 years after resection, noncancer-specific CID was higher than lung cancer-specific CID; the higher noncancer-specific, early-phase mortality was enhanced in patients ≥ 75 years of age than in those 65 to 74 years of age. Multivariable analysis showed that low ppo diffusing capacity of lung for carbon monoxide was an independent predictor of severe morbidity ( P < .001), 1-year mortality ( P < .001), and noncancer-specific mortality ( P < .001), whereas low ppo forced expiratory volume in 1 second was an independent predictor of lung cancer-specific mortality ( P = .002). Conclusion In patients who undergo curative-intent resection of stage I NSCLC, noncancer-specific mortality is a significant competing event, with an increasing impact as patient age increases.
Figures
Comment in
-
Tailored Therapy for Stage I Non-Small-Cell Lung Cancer.J Clin Oncol. 2017 Jan 20;35(3):268-270. doi: 10.1200/JCO.2016.70.4718. Epub 2016 Nov 14. J Clin Oncol. 2017. PMID: 27937087 No abstract available.
-
Moving beyond disease-focused decision making: understanding competing risks to personalize lung cancer treatment for older adults.J Thorac Dis. 2017 Jan;9(1):8-12. doi: 10.21037/jtd.2017.01.36. J Thorac Dis. 2017. PMID: 28203399 Free PMC article. No abstract available.
-
The Head Start Effect: Will Acute and Delayed Postoperative Mortality Lead to Improved Survival with Stereotactic Body Radiation Therapy for Operable Stage I Non-Small-Cell Lung Cancer?J Clin Oncol. 2017 May 20;35(15):1749-1751. doi: 10.1200/JCO.2016.72.0003. Epub 2017 Feb 21. J Clin Oncol. 2017. PMID: 28221860 No abstract available.
-
Reply to C.G. Rusthoven et al.J Clin Oncol. 2017 May 20;35(15):1751-1752. doi: 10.1200/JCO.2016.72.0029. Epub 2017 Feb 21. J Clin Oncol. 2017. PMID: 28221863 No abstract available.
-
Analyzing competing risks in the treatment of lung cancer: a good start.J Thorac Dis. 2017 Mar;9(3):474-476. doi: 10.21037/jtd.2017.02.96. J Thorac Dis. 2017. PMID: 28449448 Free PMC article. No abstract available.
References
-
- Stat Bite Percentage of New Cases by Age Group For Lung and Bronchus Cancer (2008-2012). JNCI J Natl Cancer Inst 108:djw056, 2016 - PubMed
-
- Janssen-Heijnen ML, Houterman S, Lemmens VE, et al. Prognostic impact of increasing age and co-morbidity in cancer patients: A population-based approach. Crit Rev Oncol Hematol. 2005;55:231–240. - PubMed
-
- NCCN clinical practice guidelines in oncology (NCCN Guidelines): Non-small cell lung cancer version 2.2016. Ft Washington, PA, National Comprehensive Cancer Network, 2016
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
