

Tenascin-C and fibronectin expression divide early stage tongue cancer into low- and high-risk groups
- PMID: 28095396
- PMCID: PMC5344290
- DOI: 10.1038/bjc.2016.455
Tenascin-C and fibronectin expression divide early stage tongue cancer into low- and high-risk groups
Abstract
Background: Oral tongue squamous cell carcinoma (OTSCC) metastasises early, especially to regional lymph nodes. There is an ongoing debate on which early stage (T1-T2N0) patients should be treated with elective neck dissection. We need prognosticators for early stage tongue cancer.
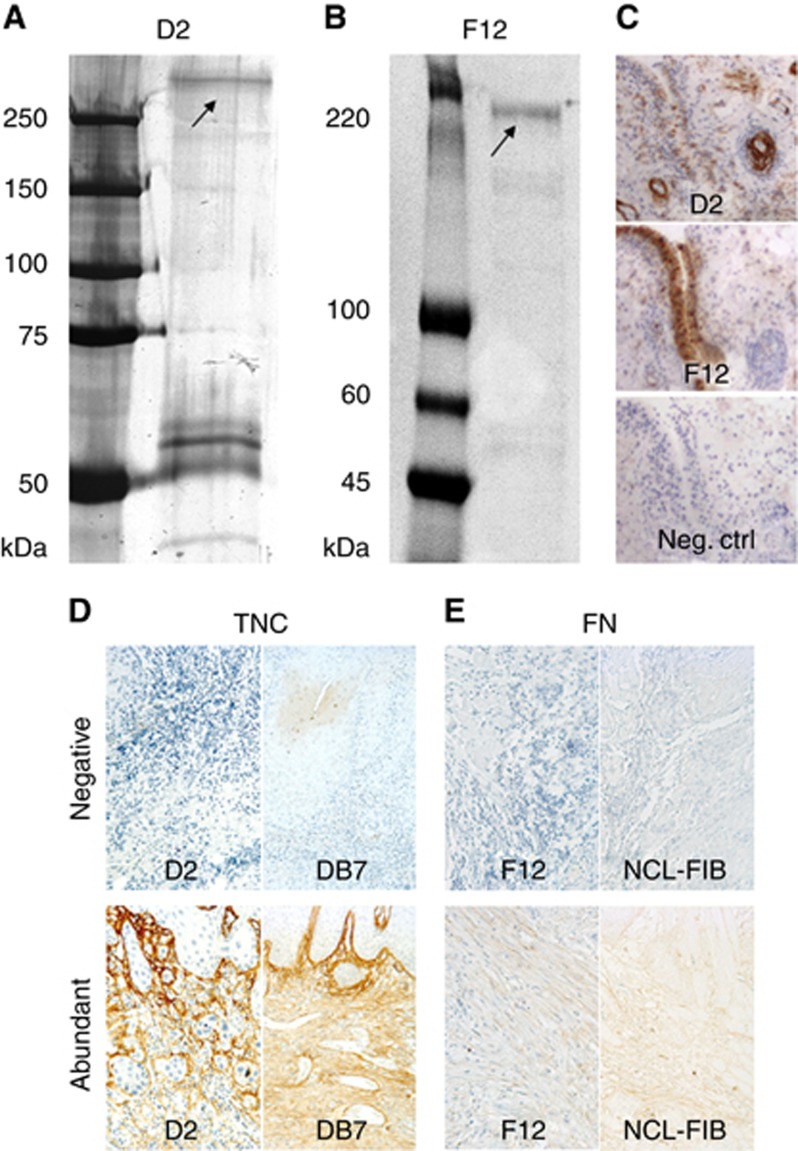
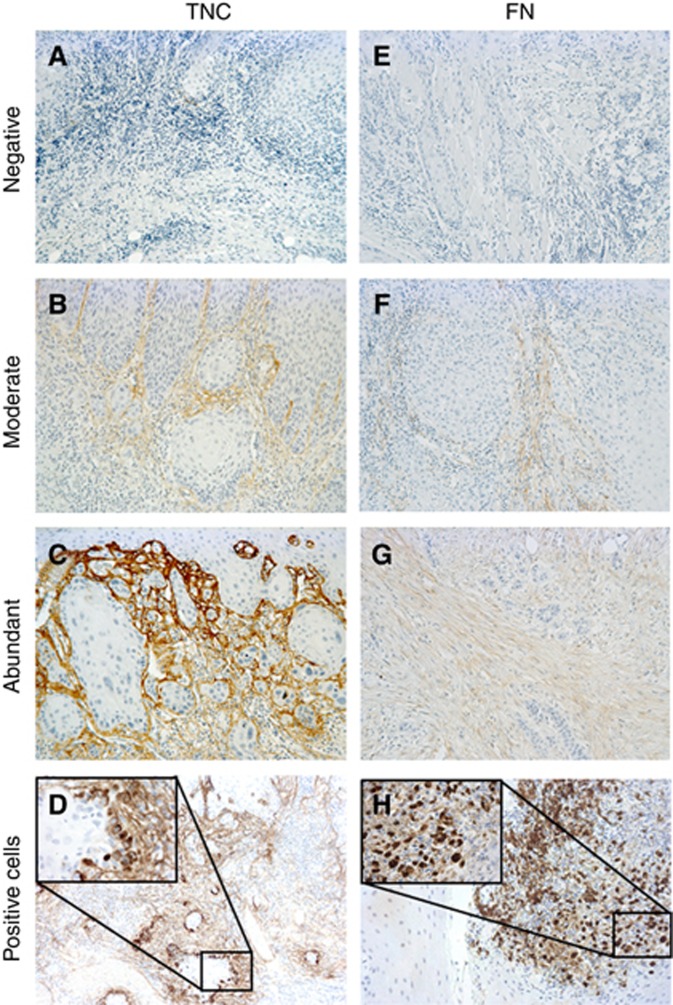
Methods: Mice immunisation with human mesenchymal stromal cells resulted in production of antibodies against tenascin-C (TNC) and fibronectin (FN), which were used to stain 178 (98 early stage), oral tongue squamous cell carcinoma samples. Tenascin-C and FN expression in the stroma (negative, moderate or abundant) and tumour cells (negative or positive) were assessed. Similar staining was obtained using corresponding commercial antibodies.
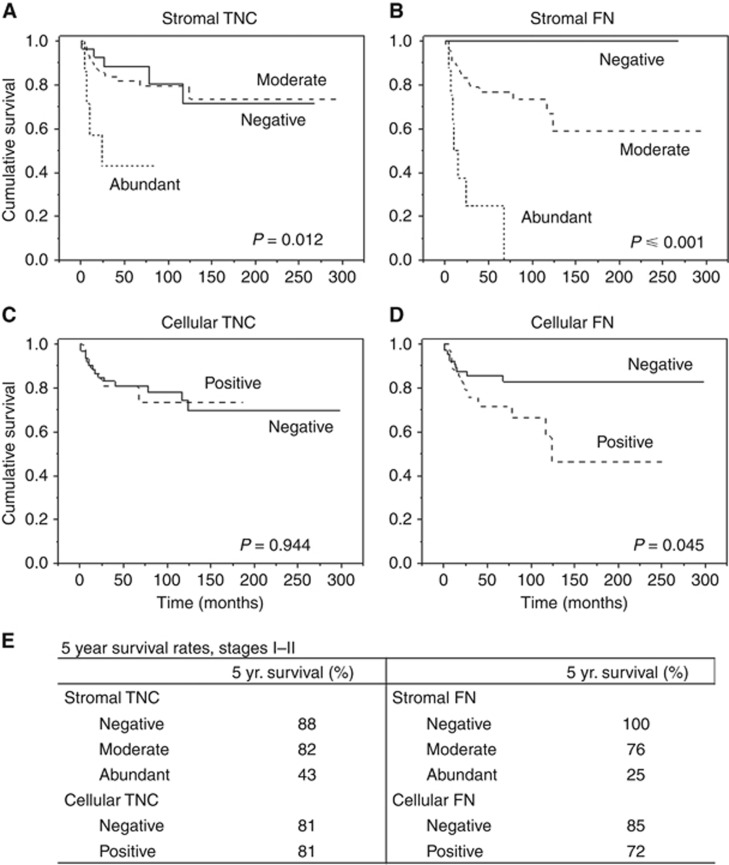
Results: Expression of TNC and FN in the stroma, but not in the tumour cells, proved to be excellent prognosticators both in all stages and in early stage cases. Among early stages, when stromal TNC was negative, the 5-year survival rate was 88%. Correspondingly, when FN was negative, no cancer deaths were observed. Five-year survival rates for abundant expression of TNC and FN were 43% and 25%, respectively.
Conclusions: Stromal TNC and, especially, FN expressions differentiate patients into low- and high-risk groups. Surgery alone of early stage primary tumours might be adequate when stromal FN is negative. Aggressive treatments should be considered when both TNC and FN are abundant.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Al Moustafa A-E, Alaoui-Jamali MA, Batist G, Hernandez-Perez M, Serruya C, Alpert L, Black MJ, Sladek R, Foulkes WD (2002) Identification of genes associated with head and neck carcinogenesis by cDNA microarray comparison between matched primary normal epithelial and squamous carcinoma cells. Oncogene 21(17): 2634–2640. - PubMed
-
- Almangush A, Bello IO, Keski-Säntti H, Mäkinen LK, Kauppila JH, Pukkila M, Hagström J, Laranne J, Tommola S, Nieminen O, Soini Y, Kosma V-M, Koivunen P, Grénman R, Leivo I, Salo T (2014) Depth of invasion, tumor budding, and worst pattern of invasion: prognostic indicators in early-stage oral tongue cancer. Head Neck 36(6): 811–818. - PMC - PubMed
-
- Bagordakis E, Sawazaki-Calone I, Macedo CC, Carnielli CM, de Oliveira CE, Rodrigues PC, Rangel AL, Dos Santos JN, Risteli J, Graner E, Salo T, Leme AF, Coletta RD (2016) Secretome profiling of oral squamous cell carcinoma-associated fibroblasts reveals organization and disassembly of extracellular matrix and collagen metabolic process signatures. Tumour Biol 37(7): 9045–9057. - PubMed
-
- Barnes L, Eveson JW, Reichart P, Sidransky D (2005) Pathology and Genetics of Head and Neck Tumours. IARC Press: Lyon.
-
- Bello IO, Soini Y, Salo T (2010) Prognostic evaluation of oral tongue cancer: means, markers and perspectives (I). Oral Oncol 46(9): 630–635. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
