

Intensive versus Guideline Blood Pressure and Lipid Lowering in Patients with Previous Stroke: Main Results from the Pilot 'Prevention of Decline in Cognition after Stroke Trial' (PODCAST) Randomised Controlled Trial
- PMID: 28095412
- PMCID: PMC5240987
- DOI: 10.1371/journal.pone.0164608
Intensive versus Guideline Blood Pressure and Lipid Lowering in Patients with Previous Stroke: Main Results from the Pilot 'Prevention of Decline in Cognition after Stroke Trial' (PODCAST) Randomised Controlled Trial
Abstract
Background: Stroke is associated with the development of cognitive impairment and dementia. We assessed the effect of intensive blood pressure (BP) and/or lipid lowering on cognitive outcomes in patients with recent stroke in a pilot trial.
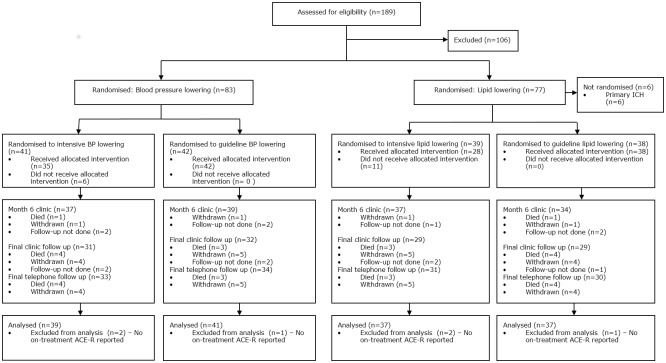
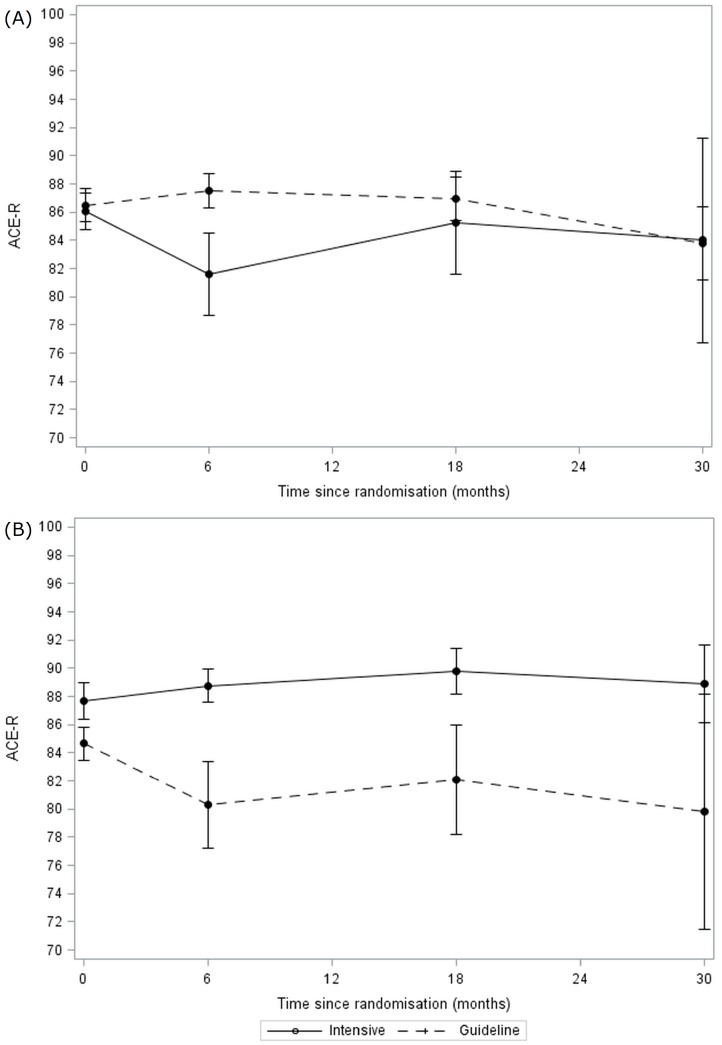
Methods: In a multicentre, partial-factorial trial, patients with recent stroke, absence of dementia, and systolic BP (SBP) 125-170 mmHg were assigned randomly to at least 6 months of intensive (target SBP <125 mmHg) or guideline (target SBP <140 mmHg) BP lowering. The subset of patients with ischaemic stroke and total cholesterol 3.0-8.0 mmol/l were also assigned randomly to intensive (target LDL-cholesterol <1.3 mmol/l) or guideline (target LDL-c <3.0 mmol/l) lipid lowering. The primary outcome was the Addenbrooke's Cognitive Examination-Revised (ACE-R).
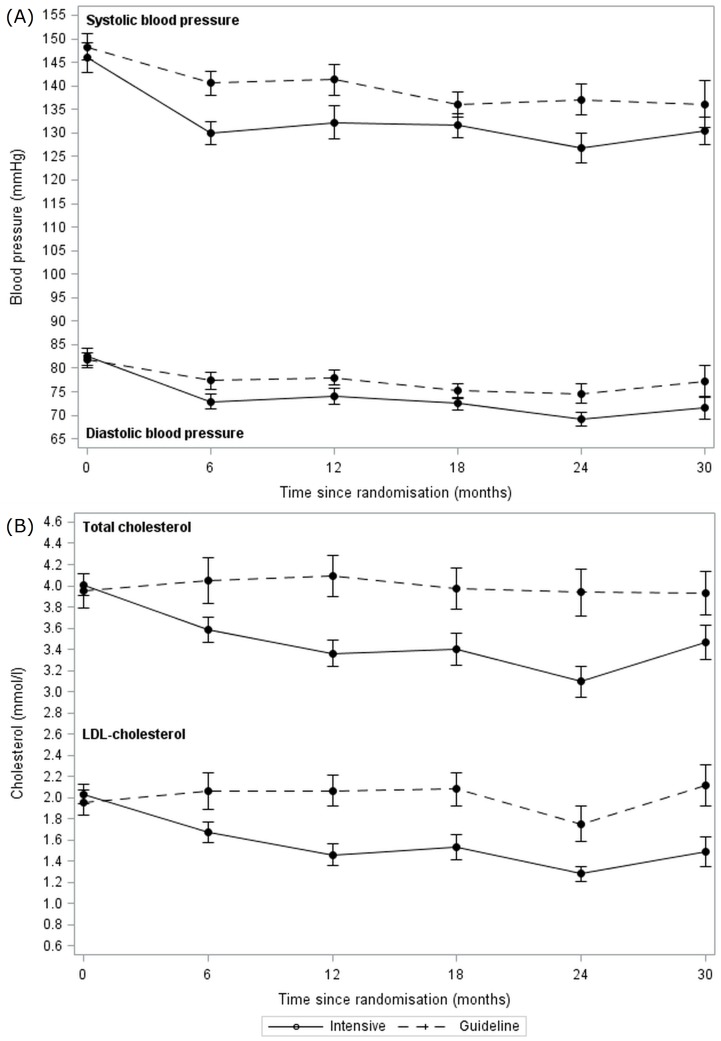
Results: We enrolled 83 patients, mean age 74.0 (6.8) years, and median 4.5 months after stroke. The median follow-up was 24 months (range 1-48). Mean BP was significantly reduced with intensive compared to guideline treatment (difference -10·6/-5·5 mmHg; p<0·01), as was total/LDL-cholesterol with intensive lipid lowering compared to guideline (difference -0·54/-0·44 mmol/l; p<0·01). The ACE-R score during treatment did not differ for either treatment comparison; mean difference for BP lowering -3.6 (95% CI -9.7 to 2.4), and lipid lowering 4.4 (95% CI -2.1 to 10.9). However, intensive lipid lowering therapy was significantly associated with improved scores for ACE-R at 6 months, trail making A, modified Rankin Scale and Euro-Qol Visual Analogue Scale. There was no difference in rates of dementia or serious adverse events for either comparison.
Conclusion: In patients with recent stroke and normal cognition, intensive BP and lipid lowering were feasible and safe, but did not alter cognition over two years. The association between intensive lipid lowering and improved scores for some secondary outcomes suggests further trials are warranted.
Trial registration: ISRCTN ISRCTN85562386.
Conflict of interest statement
PMB CB AB JM PP SP JR RS JMW GAF were grant holders for the trial with funding from Alzheimer's Society and Stroke Association. Listing the grant holders does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
