

Body Mass Index at Accession and Incident Cardiometabolic Risk Factors in US Army Soldiers, 2001-2011
- PMID: 28095509
- PMCID: PMC5241140
- DOI: 10.1371/journal.pone.0170144
Body Mass Index at Accession and Incident Cardiometabolic Risk Factors in US Army Soldiers, 2001-2011
Abstract
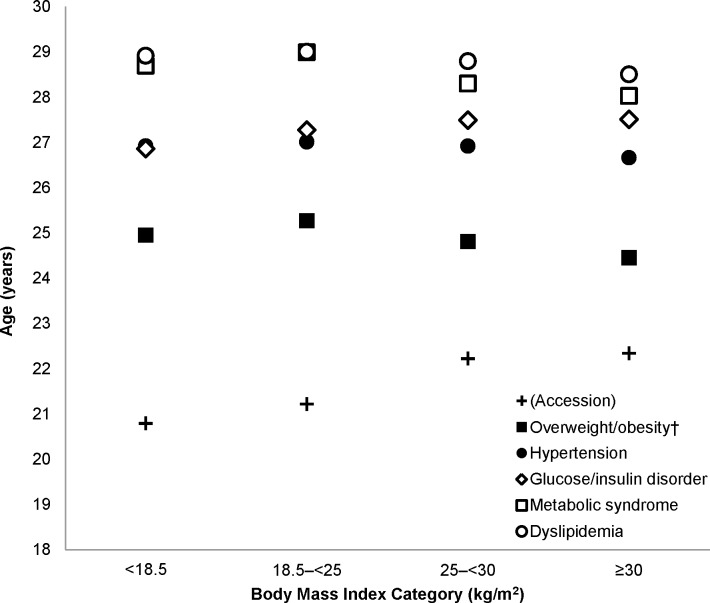
Individuals entering US Army service are generally young and healthy, but many are overweight, which may impact cardiometabolic risk despite physical activity and fitness requirements. This analysis examines the association between Soldiers' BMI at accession and incident cardiometabolic risk factors (CRF) using longitudinal data from 731,014 Soldiers (17.0% female; age: 21.6 [3.9] years; BMI: 24.7 [3.8] kg/m2) who were assessed at Army accession, 2001-2011. CRF were defined as incident diagnoses through 2011, by ICD-9 code, of metabolic syndrome, glucose/insulin disorder, hypertension, dyslipidemia, or overweight/obesity (in those not initially overweight/obese). Multivariable-adjusted proportional hazards models were used to estimate hazard ratios (HR) and 95% confidence intervals (CI) between BMI categories at accession and CRF. Initially underweight (BMI<18.5 kg/m2) were 2.4% of Soldiers, 53.5% were normal weight (18.5-<25), 34.2% were overweight (25-<30), and 10.0% were obese (≥30). Mean age range at CRF diagnosis was 24-29 years old, with generally low CRF incidence: 228 with metabolic syndrome, 3,880 with a glucose/insulin disorder, 26,373 with hypertension, and 13,404 with dyslipidemia. Of the Soldiers who were not overweight or obese at accession, 5,361 were eventually diagnosed as overweight or obese. Relative to Soldiers who were normal weight at accession, those who were overweight or obese, respectively, had significantly higher risk of developing each CRF after multivariable adjustment (HR [95% CI]: metabolic syndrome: 4.13 [2.87-5.94], 13.36 [9.00-19.83]; glucose/insulin disorder: 1.39 [1.30-1.50], 2.76 [2.52-3.04]; hypertension: 1.85 [1.80-1.90], 3.31 [3.20-3.42]; dyslipidemia: 1.81 [1.75-1.89], 3.19 [3.04-3.35]). Risk of hypertension, dyslipidemia, and overweight/obesity in initially underweight Soldiers was 40%, 31%, and 79% lower, respectively, versus normal-weight Soldiers. BMI in early adulthood has important implications for cardiometabolic health, even within young, physically active populations.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hruby A, Hu FB. The Epidemiology of Obesity: A Big Picture. PharmacoEconomics [Internet]. 2014 Dec 4 [cited 2014 Dec 8]; Available from: http://link.springer.com/10.1007/s40273-014-0243-x - DOI - PMC - PubMed
-
- U.S. Department of the Army. Army Regulation 40–501: Standards of Medical Fitness [Internet]. U.S. Department of the Army, Washington, D.C.; [cited 2014 Apr 1]. Available from: http://armypubs.army.mil/epubs/40_Series_Collection_1.html
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
