

Renal function in patients with non-dialysis chronic kidney disease receiving intravenous ferric carboxymaltose: an analysis of the randomized FIND-CKD trial
- PMID: 28095881
- PMCID: PMC5240256
- DOI: 10.1186/s12882-017-0444-6
Renal function in patients with non-dialysis chronic kidney disease receiving intravenous ferric carboxymaltose: an analysis of the randomized FIND-CKD trial
Abstract
Background: Preclinical studies demonstrate renal proximal tubular injury after administration of some intravenous iron preparations but clinical data on renal effects of intravenous iron are sparse.
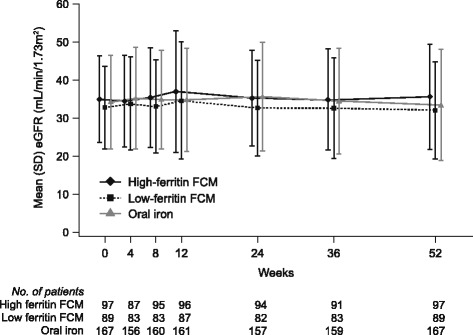
Methods: FIND-CKD was a 56-week, randomized, open-label, multicenter study in which patients with non-dialysis dependent chronic kidney disease (ND-CKD), anemia and iron deficiency without erythropoiesis-stimulating agent therapy received intravenous ferric carboxymaltose (FCM), targeting either higher (400-600 μg/L) or lower (100-200 μg/L) ferritin values, or oral iron.
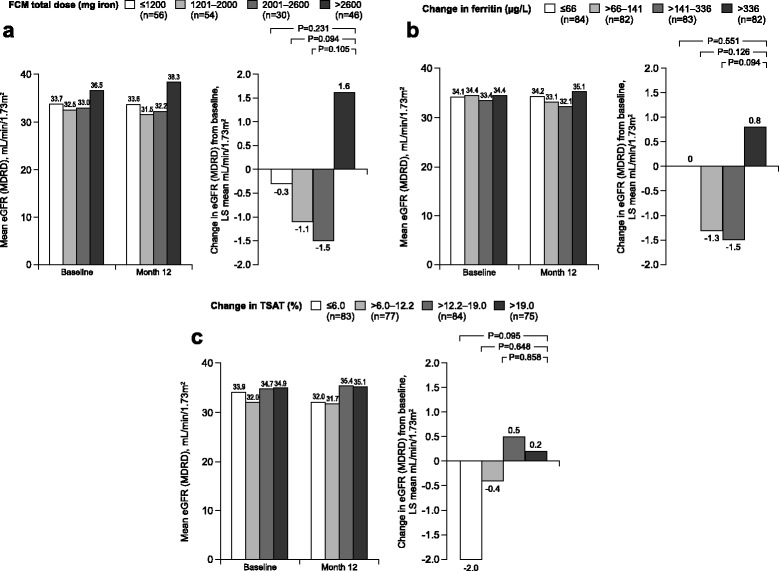
Results: Mean (SD) eGFR at baseline was 34.9 (11.3), 32.8 (10.8) and 34.2 (12.3) mL/min/1.73 m2 in the high ferritin FCM (n = 97), low ferritin FCM (n = 89) and oral iron (n = 167) groups, respectively. Corresponding values at month 12 were 35.6 (13.8), 32.1 (12.7) and 33.4 (14.5) mL/min/1.73 m2. The pre-specified endpoint of mean (SE) change in eGFR from baseline to month 12 was +0.7 (0.9) mL/min/1.73 m2 with high ferritin FCM (p = 0.15 versus oral iron), -0.9 (0.9) mL/min/1.73 m2 with low ferritin FCM (p = 0.99 versus oral iron) and -0.9 (0.7) mL/min/1.73 m2 with oral iron. No significant association was detected between quartiles of FCM dose, change in ferritin or change in TSAT versus change in eGFR. Dialysis initiation was similar between groups. Renal adverse events were rare, with no indication of between-group differences.
Conclusion: Intravenous FCM at doses that maintained ferritin levels of 100-200 μg/L or 400-600 μg/L did not negatively impact renal function (eGFR) in patients with ND-CKD over 12 months versus oral iron, and eGFR remained stable. These findings show no evidence of renal toxicity following intravenous FCM over a 1-year period.
Trial registrations: ClinicalTrials.gov NCT00994318 (first registration 12 October 2009).
Keywords: Chronic kidney disease; Ferinject; Ferric carboxymaltose; Intravenous; Renal function; eGFR.
Figures
References
-
- Solomon SE, Uno H, Lewis EF, Eckardt KU, Lin J, Burdmann EA, de Zeeuw D, Ivanovich P, Levey AS, Parfrey P, Remuzzi G, Singh AK, Toto R, Huang F, Rossert J, McMurray JJ, Pfeffer MA. Trial to Reduce Cardiovascular Events with Aranesp Therapy (TREAT) Investigators. Erythropoietic response and outcomes in kidney disease and type 2 diabetes. N Engl J Med. 2010;363:1146–1155. doi: 10.1056/NEJMoa1005109. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
