

Efficacy and Safety of Apixaban Compared With Warfarin in Patients With Atrial Fibrillation and Peripheral Artery Disease: Insights From the ARISTOTLE Trial
- PMID: 28096100
- PMCID: PMC5523640
- DOI: 10.1161/JAHA.116.004699
Efficacy and Safety of Apixaban Compared With Warfarin in Patients With Atrial Fibrillation and Peripheral Artery Disease: Insights From the ARISTOTLE Trial
Abstract
Background: We studied (1) the rates of stroke or systemic embolism and bleeding in patients with atrial fibrillation and peripheral artery disease (PAD) and (2) the efficacy and safety of apixaban versus warfarin in patients with atrial fibrillation with and without PAD.
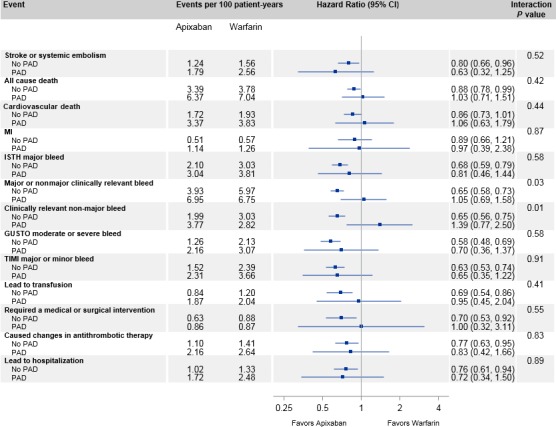
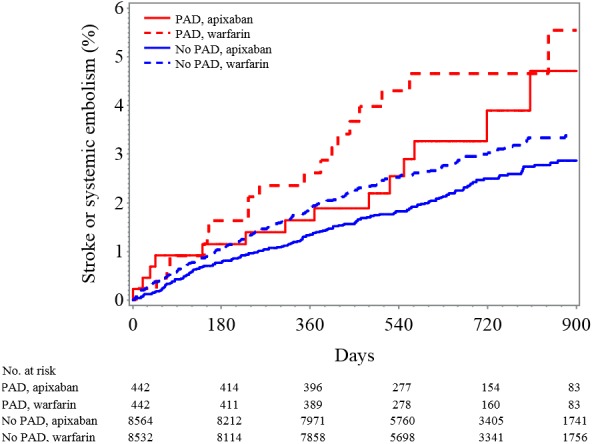
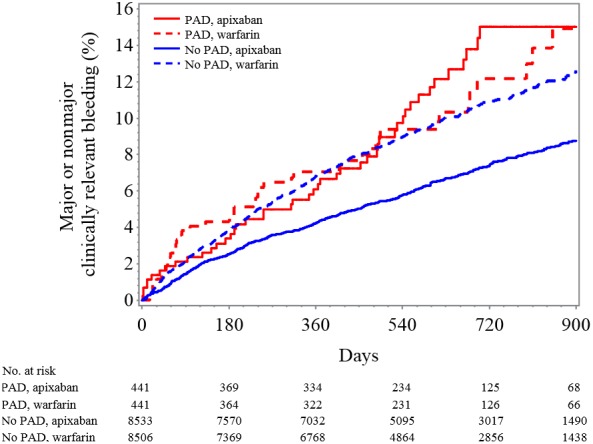
Methods and results: The Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial randomized 18 201 patients with atrial fibrillation to apixaban or warfarin for stroke/systemic embolism prevention; 884 (4.9%) patients had PAD at baseline. Patients with PAD had higher unadjusted rates of stroke and systemic embolism (hazard ratio [HR] 1.73, 95% CI 1.22-2.45; P=0.002) and major bleeding (HR 1.34, 95% CI 1.00-1.81; P=0.05), but after adjustment, no differences existed in rates of stroke and systemic embolism (HR 1.32, 95% CI 0.93-1.88; P=0.12) and major bleeding (HR 1.03, 95% CI 0.76-1.40; P=0.83) compared with patients without PAD. The risk of stroke or systemic embolism was similar in patients assigned to apixaban and warfarin with PAD (HR 0.63, 95% CI 0.32-1.25) and without PAD (HR 0.80, 95% CI 0.66-0.96; interaction P=0.52). Patients with PAD did not have a statistically significant reduction in major or clinically relevant nonmajor bleeding with apixaban compared with warfarin (HR 1.05, 95% CI 0.69-1.58), whereas those without PAD had a statistically significant reduction (HR 0.65, 95% CI 0.58-0.73; interaction P=0.03).
Conclusions: Patients with PAD in ARISTOTLE had a higher crude risk of stroke or systemic embolism compared with patients without PAD that was not present after adjustment. The benefits of apixaban versus warfarin for stroke and systemic embolism were similar in patients with and without PAD. These findings highlight the need to optimize the treatment of patients with atrial fibrillation and PAD.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00412984.
Keywords: apixaban; atrial fibrillation; bleeding; peripheral artery disease; stroke; systemic embolism.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, Gillum RF, Kim YH, McAnulty JH Jr, Zheng ZJ, Forouzanfar MH, Naghavi M, Mensah GA, Ezzati M, Murray CJ. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129:837–847. - PMC - PubMed
-
- Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA, Criqui MH. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–1340. - PubMed
-
- Hijazi Z, Lindbäck J, Alexander JH, Hanna M, Held C, Hylek EM, Lopes RD, Oldgren J, Siegbahn A, Stewart RA, White HD, Granger CB, Wallentin L. The ABC (age, biomarkers, clinical history) stroke risk score: a biomarker‐based risk score for predicting stroke in atrial fibrillation. Eur Heart J. 2016;37:1582–1590. - PMC - PubMed
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor‐based approach: the Euro Heart Survey on atrial fibrillation. Chest. 2010;137:263–272. - PubMed
-
- Olesen JB, Lip GY, Lane DA, Køber L, Hansen ML, Karasoy D, Hansen CM, Gislason GH, Torp‐Pedersen C. Vascular disease and stroke risk in atrial fibrillation: a nationwide cohort study. Am J Med. 2012;125:826. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
